- Research
- Open access
- Published:
Challenges in accessing health care services for women and girls with disabilities using a humanitarian physical rehabilitation program in Lebanon: a mixed method study
International Journal for Equity in Health volume 23, Article number: 267 (2024)
Abstract
Background
Achieving equitable healthcare access for persons with disabilities is vital, as they often face various barriers that impact their health and well-being. Recognizing the importance of gender equity, this study aims to explore the specific barriers faced by women and girls with disabilities in accessing quality healthcare services in Lebanon.
Methods
A mixed-method sequential explanatory approach was employed. Initially, a retrospective descriptive study analyzed data from the International Committee of the Red Cross (ICRC)-supported physical rehabilitation programme (PRP) database. Subsequently, in-depth interviews were conducted to delve into factors influencing gender-disproportionate service users and to uncover barriers to accessing healthcare. Levesque et al.‘s ‘Conceptual framework on healthcare access’ was used to organize and map the results.
Results
The quantitative analysis of service utilization at ICRC PRP centers from 2015 to 2022 revealed significant gender disparities, with males comprising 66.6% of service users compared to 33.4% females. This trend was consistent across age categories, nationalities, and clinical conditions. Healthcare access for women and girls with disabilities was found to be inadequate across all five dimensions of the Levesque framework: adequacy, accessibility, affordability, appropriateness, and availability, as well as their corresponding abilities. While certain challenges such as transportation, financial constraints, inadequate infrastructure, and limited information on available services were common to both genders, gender-specific barriers primarily included societal norms, safety concerns during unaccompanied visits to healthcare facilities, limited access to societal information, economic disparities, preferences for female healthcare providers, and the need for privacy during consultations.
Conclusion
This study underscores key barriers hindering healthcare access for women and girls with disabilities in Lebanon, necessitating tailored interventions. Gender-specific challenges, including societal norms and safety concerns, require targeted solutions for improved access and outcomes. This study serves as a call to action for stakeholders at various levels to collaborate and implement concrete measures to bridge the gap in healthcare access and ensure that no one is left behind.
Introduction
Disabilities disproportionately affect women and girls, particularly in low- and middle-income countries (LMICs), where they are estimated to represent approximately 75% of persons with disabilities [1]. Gender and disability are intersecting determinants of vulnerability because they influence access to resources, health-seeking patterns, and autonomy in decision-making around health. Women with disabilities are approximately three times more likely to have unmet healthcare needs than men due to both gender- and disability-related barriers while seeking, paying for, and receiving necessary healthcare [2].
In conflict-affected and humanitarian settings, displacement, both internally and cross- border, is a further intersecting factor in the cumulative challenges faced by women and girls with disabilities. Across their journey, women and girls typically face reduced safety, a risk of violence or injury, unmet basic needs, a lack of resources, encounters of discrimination and psychological distress, reproductive health risks, and a lack of access to basic healthcare and support services [3].
Although physical, sensory, intellectual and mental disabilities can occur, the focus of this research is on physical disability, which is defined as a disability associated with a physical impairment that affects an individual’s mobility, coordination, dexterity, or other physical functions [4, 5]. Data from 38 physical rehabilitation centers in humanitarian settings between 1988 and 2018 indicate disproportionate service use by men, with women representing less than 20% of the case load [5]. The lower service utilization in these settings suggests a high level of unmet need and the need for more comprehensive and contextual knowledge of the factors that might influence health-seeking behaviors and access to health care services. This view is in line with the global literature on gender and rehabilitation, which indicates greater care needs, more limited access, use, and continued adherence, and worse outcomes among women than among men, although these trends emerge predominantly from high-income countries [3].
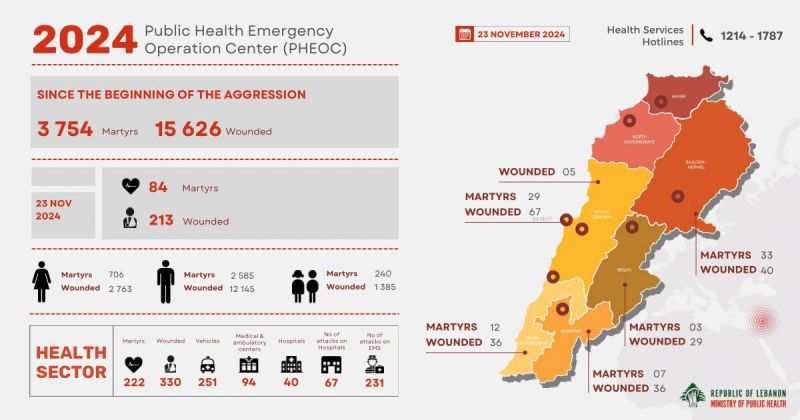
LMICs in general and conflict-affected settings in particular are often affected by compounded challenges that can exacerbate preexisting vulnerabilities [6]. Lebanon was recently classified by the World Bank as an LMIC [7], and over the past years, it has faced a multifaceted crisis involving economic, sociopolitical, security, and public health issues. The situation is further worsened by a political deadlock, increased instability, and the enduring impact of the Port of Beirut Blast, which resulted in extensive destruction, displacement, and injuries to approximately 7,000 people [8, 9]. Today, the picture is further compounded by an ongoing armed conflict that is disproportionately harming civilians with almost 4’000 dead and over 15’000 wounded at the times of writing, according to the Lebanese Ministry of Public Health [10]. In this challenging context, persons with disabilities often face barriers in accessing fundamental services such as education, health, and social support; enduring discrimination; and an elevated risk of abuse, particularly among women and girls [11]. In contrast to global trends suggesting a higher prevalence of disability in women, Lebanon’s local data reveal a discrepancy. A recent report showed similar proportions of men and women with disabilities, with very few differences in terms of disability type [12]. That being said, approximately 400,000 individuals in the country hold disability cards issued by the Ministry of Social Affairs (MoSA), represented predominantly by men. Identification at MoSA-run Social Development Centers relies on a medical approach that prioritizes observational verification of physical disabilities, potentially excluding those with ‘hidden’ disabilities [13].
Efforts to ensure equitable access to healthcare services for persons with disabilities in Lebanon are crucial, particularly in light of the financial crisis and the need for comprehensive support to those most vulnerable in the population. Acknowledging the crucial role of women and their entitlement to equal participation in healthcare systems, there is a need to have a deeper understanding of the barriers faced by women and girls with disabilities and their coping strategies in accessing safe and high-quality healthcare services [14].
The present study was designed with the aim of providing an in-depth understanding of the nature and diversity of obstacles experienced by women and girls with physical disabilities to access healthcare services in Lebanon. Using secondary quantitative data of service users of the International Committee of the Red Cross (ICRC) supported physical rehabilitation centers, this study seeks to describe the demographic characteristics of persons with disabilities attending these centers. Through in-depth interviews, this study aimed to identify the key barriers experienced by women and girls with physical disabilities served by ICRC-supported facilities in accessing healthcare services within the broader health care system in which these facilities operate. We highlight the voice, aspirations, and preferences of women and girls with disabilities and aim to use their inputs and narratives to design interventions that can address their health-seeking barriers and challenges.
Methods
Study design
A sequential explanatory mixed method approach was considered appropriate for generating insights from the existing statistics of service users, with qualitative explorations in a purposefully sampled group to better understand the experiences and needs of women and girls with disabilities in Lebanon. First, a retrospective descriptive study was conducted on aggregated data from the ICRC physical rehabilitation program (PRP) database in Lebanon, encompassing persons with disabilities who sought physical rehabilitation services between 2015 and 2022. This was followed by in-depth interviews to understand the factors that can contribute to disproportionate gender service use and to identify the barriers faced by women and girls with physical disabilities in accessing health care services.
Study setting
The ICRC PRP in Lebanon was established in 2015 to support the national health system in absorbing the increased demand for services observed following the influx of refugees fleeing the conflict in neighboring Syria. The ICRC’s services aim to empower persons with permanent impairments, facilitating their ability to lead productive and autonomous lives with dignity. From its inception in 2015 until December 2022, the program has provided services to more than 6000 people in five ICRC PRP-supported centers in Lebanon. The range of services offered by the ICRC PRP included prosthetic and orthotic fittings, physiotherapy sessions, wheelchair services, and the provision of mobility devices. Moreover, the PRP operates within a broader network of health service providers, and systematically adopts a continuum-of-care approach through defining referral pathways across promotive, preventive, curative, rehabilitative, and palliative services at the primary, secondary, and tertiary level of care. Additionally, the ICRC provides and advocates for inclusive humanitarian services and serves as a disability-inclusive employer. This approach creates and supports opportunities for persons with disabilities to realize their full potential in societies affected by armed conflict and other situations of violence.
Ethical considerations
Ethical approval for this study was granted by the International Committee of the Red Cross (ICRC) Ethical Review Board under the reference number LDP_CORE 23/00007 - CGB/bap. The research was conducted in accordance with the principles outlined in the Declaration of Helsinki. For the retrospective descriptive study, service users were obtained from the ICRC PRP database and analyzed anonymously. Therefore, informed consent was not required for this part of the study. However, for the qualitative component, each participant was provided written information with details of the study. This ensured their understanding of their rights, including voluntary participation and the right to withdraw consent at any point. Additionally, participants were assured that their decision to participate, whether positive or negative, would not impact their regular access to services. Written informed consent was obtained through a straightforward Yes/No question, giving participants the option to decline audio recording while still being able to participate in the study. To safeguard data confidentiality, all information was securely stored on a password-protected laptop and made accessible solely to the research team for study-related purposes.
Data collection
Secondary data analysis of service users
As part of routine data collection at the ICRC, service user information is systematically recorded and managed in a Microsoft Excel spreadsheet. The dataset underwent a thorough process of data cleaning, merging, and aggregation. We retrieved data on age, sex, nationality, and main clinical conditions. Age was categorized into five categories: young child (younger than 5 years), child (5–17 years), young adult (18–34 years), adult (35–59 years), and older adult (older than 59 years). The main clinical conditions necessitating ICRC PRP services were broadly classified into two categories: amputation and other physical disability types. Descriptive statistics were used to summarize the data, with frequencies and percentages reported for categorical variables. Chi-square or Fischer exact tests were conducted to examine gender differences across age categories, nationality, and clinical conditions. Statistical analyses were conducted using IBM SPSS v.26, with significance set at a p value less than 0.05.
In-depth interviews with women and girls with disabilities
Sampling frame and procedure
Participants were purposively sampled from the PRP admission/coverage criteria of the ICRC, and only women and caregivers/parents of girls aged less than 18 years with physical disability were selected for interviews. The exclusion criteria were as follows: women or caregivers unable to provide informed consent, and individuals with severe cognitive impairments that limited effective communication during the interviews.
Eighteen participants were selected to represent different nationalities and residency areas, including Beirut and North Lebanon. The 18 participants comprised 9 women and 9 girls, representing different nationalities, including Lebanese, Palestinian, and Syrian. Within this group, there were 9 caregivers of girls with physical disabilities who were evenly distributed among Lebanese refugees, Syrian refugees, and Palestinian refugees. Additionally, there were 7 women with physical disabilities, including 3 Lebanese refugees, 2 Syrian refugees, and 2 Palestinian refugees. Furthermore, 2 caregivers of women with physical disabilities were included, one Syrian and the other Palestinian. Among the caregivers, there were 4 mothers, 3 fathers, and 2 sons, reflecting a variety of familial roles and relationships within the caregiving context. Recruitment took place over 6 weeks from February to March 2023.
Qualitative data collection
Women and caregivers were contacted by a female master’s student in public health at the ICRC and two ICRC PRP staff via phone calls. Participants were invited to participate in the study, and during the invitation, the purpose and time of the interview were explained. The interviews were scheduled to take place in a private meeting room at the ICRC offices. Before starting the interviews, the three investigators provided an information sheet and written consent form to the participants, which explained the purpose and scope of the study, the use of data, privacy considerations, and data management concerns. The consent form ensured that the participants understood the study and voluntarily agreed to participate.
Two interview guides were developed containing semi structured and open-ended questions. One guide was intended for women with physical disabilities, while the other was for caregivers of girls under 18 years with physical disabilities (Supplementary file Appendix 1). Each guide was tailored to address the specific needs and experiences of these distinct groups. These interview guides were created by a research team member who had extensive experience working with persons with disabilities in Lebanon. The interview questions covered various topics, including barriers and challenges faced while accessing healthcare, accessible healthcare services, feedback mechanisms, and suggestions to reduce these barriers. These topics support a broad understanding of healthcare access issues across different settings. Notably, the interview guides were originally developed in English and subsequently translated into Arabic. The interviews lasted between 30 and 40 min, and they were recorded using an ICRC laptop. During the interviews, the interviewers were attentive to signs of distress, fatigue, or any indication of the need for urgent medical attention. If any such signs were observed, the interviewers promptly referred the relevant details to the ICRC staff to organize necessary care for the participants. The participants received a transportation stipend, likely to cover their travel expenses related to attending the interviews.
Data analysis
The data was analyzed using a deductive-inductive approach with the utilization of Levesque et al.‘s ‘Conceptual framework on health care access’ for interpreting our findings. The audio-recorded interviews were transcribed verbatim in Arabic. Thematic analysis was performed following Braun and Clark’s (2006) six-step guide: (1) becoming familiar with the data, (2) generating initial codes, (3) searching for themes, (4) reviewing themes, (5) defining and naming themes, and (6) producing the final report. We then retrospectively applied Levesque et al.‘s ‘Conceptual framework on health care access’ to analyze our data. Developed by Levesque and colleagues, this framework provides a comprehensive theoretical model for understanding access to health care services. It comprises five main dimensions, namely, adequacy, accessibility, affordability, appropriateness, and availability, which are essential for assessing the complex interplay of factors influencing health care access. Additionally, the framework delineates five equivalent abilities of population groups: ability to perceive, ability to seek, ability to reach, ability to pay, and ability to engage, reflecting the diverse experiences and challenges individuals may face in accessing health care (Fig. 1) [15, 16].

Levesque conceptual framework for healthcare access [14]
While our research initially did not intend to utilize this framework, we found it to be a valuable tool for interpreting our findings in the context of access to health care. By applying the framework, a posteriori, we were able to examine various dimensions of health care access and understand how they intersected with our study outcomes. This approach allowed us to gain deeper insights into the factors influencing access to health care in our study population and facilitated comparisons with literature. Only quotes used in reporting findings were translated to the English language. Two independent bilingual specialists checked the quality of the translations from Arabic to English.
Results
Quantitative analysis of PRP service use
Table 1 offers a comprehensive overview of the total number of users by sex from 2015 to 2022. Over this seven-year span, a total of 6680 persons with disabilities received ICRC PRP services, 33.4% of whom were females and 66.6% of whom were males.
A chi-square test revealed a statistically significant male predominance across all age categories (p value = 0.004) (Supplementary file Appendix 2).
Figure 2 provides an overview of the sex distribution trends in accessing PRP services among different nationalities from 2015 to 2020.

Sex distribution in accessing ICRC PRP services by nationality between 2015 and 2020. NB: Data on nationalities were available for the period from 2015 to 2020
Among all nationalities, a predominant male representation is observed across all age categories, with the notable exception of Palestinian young adults (18–34 y), where the female group constitutes 63% of service users (Table 2).
The main reasons for attending the centers over the study period were amputation (28.1%), cerebral palsy (19.8%), congenital deformity (12.3%), clubfoot (2.1%) and others (37.3%). Figure 4 provides an overview of the amputation-related sex distribution in PRP service access between 2015 and 2022. In the amputee cohort, the sex imbalance was particularly pronounced, with 80.9% being males and 19.1% being females. A chi-square test revealed that among the other physical disability types, men consistently constituted a significantly larger portion, comprising 61.1%, compared to 38.9% women, showcasing a persistent male majority (P-value < 0.001) (Fig. 3).

Amputation-related sex distribution in PRP service access between 2015 and 2022
The detailed examination of age and sex distributions among service users attending ICRC-supported rehabilitation centers during the same period revealed patterns that differed between those with amputation and those with other physical disability types. Among amputees, males dominate across all age groups, comprising 80.9%, with the highest prevalence observed in the young child at 91.3% and adult category (18–34 years) at 84.7%. In contrast, females with amputation exhibit a higher representation in the child group (5–17 years) and older adult group ((≥ 60 years) at 28.7%. Among those without amputation, males constitute 61.1%, with the highest representation in the young adult age group (18–34 years), accounting for 73.7%. Females, on the other hand, are more prevalent in the older age categories, with 49.4% in the older adult group aged more than 60 years old (Table 3).
Qualitative exploration of women’s and girls’ health-seeking experience and challenges
Approachability and ability to perceive
Outreach and Information availability
Access to preventative healthcare services, such as vaccinations, was reported by all participants as readily accessible to them, thanks to the outreach efforts conducted by various nongovernmental organizations (NGOs), including the Lebanese Red Cross (LRC), ICRC, and United Nations (UN) agencies. However, information on access to curative primary care at the facility level was reported to be more limited, with several participants indicating that they were unable to find the needed information when necessary. Those who were able to receive information reported receiving information from their family or community networks in the majority of cases or from their physiotherapist in some others.
Fear and health beliefs
Participants emphasized the critical importance of mobility and its prioritization over even basic needs such as food, water, and improved living conditions. This perspective underscores the foundational role of physical mobility in enabling individuals to access resources, maintain independence, and participate in daily activities. In contrast, some participants revealed psychological barriers to engaging with healthcare services. One participant expressed a fear of diagnostic procedures, such as laboratory tests, due to concerns about discovering a potential illness. This hesitancy illustrates the role of health-related anxieties in discouraging individuals from seeking preventive or routine care, even when experiencing symptoms.
Health literacy
Health literacy emerged as a pivotal factor influencing caregivers’ health-seeking behaviors and their ability to navigate the healthcare system effectively. Participants with higher health literacy demonstrated proactive and informed approaches to care. For instance, one caregiver with a professional health background leveraged her knowledge to access preventive and curative services for her children with disabilities, even independently administering over-the-counter supplements to support their recovery. This illustrates how health literacy can empower caregivers to act decisively and effectively in managing their dependents’ health. Conversely, caregivers with limited health literacy expressed confusion and uncertainty about where and how to seek appropriate care, which often hindered timely and effective health-seeking behaviors.
One caregiver, for example, reported:
“Now her Knee Ankle Foot Orthosis (KAFO) is too small for her I don’t know if it is necessary for her to continue to wear them. She used them after her surgery. We haven’t seen a doctor for a very long time.” (P9).
Spirituality
Many participants shared that they have a strong sense of faith even, which helps them be grateful for what they have and believe that a solution will come their way.
“We are relying on God and treating her. Our living situation is like everyone else; we are all living in the same situation in this country.” (P10).
Acceptability and ability to seek
No gender discrimination
No participant, whether a caregiver or girl/woman with disability, reported having been discriminated against on the basis of their gender in healthcare institutions. Some participants even suggested that women might be treated with more respect and compassion than men since they are generally calmer and have a better temper than men.
“No, no, it is all the same. I mean, men were standing waiting just like women, equally. In addition, the treatment, in fact, for men was worse than for women, just so you know. Some of the men were very tense in the health facilities we were in, and there was frustration, irritation, and stress. I mean, you feel that we, as women, have a more positive aspect in that if we are in a certain place, we are treated more politely or better.” (P1).
Societal gender discrimination
As the present study aims to gain an in-depth understanding of the nature and diversity of obstacles experienced by women and girls with physical disabilities to access healthcare services, it was important to capture any social values or gender differences that affected their access. Participants highlighted the intersection of gender and social dependency in caregiving dynamics, emphasizing how societal perceptions and norms disproportionately affect women and girls. A recurring theme was the perception that women are seen as more dependent on assistance but face fewer opportunities to receive it. For instance, caregivers noted that boys often benefit from a wider network of support, with care provided by any family member, whereas girls are typically reliant on female caregivers due to cultural norms.
“A woman is seen as less capable than a man. She is perceived as not knowing as much as a man and as being unable to rely on herself because she has a physical disability. She always needs someone with her, someone to assist her, even for basic needs such as eating. If she were a boy, it would have been easier in all aspects; girls are usually weaker than boys. A girl needs more care. A boy might have his father or brother to help him, but a girl needs her mother or sister for this matter. She requires more attention.” (P12).
“It’s a crime for a woman who has a disability to be uneducated because she will be erased from society; she will never appear to the community; she will be wronged. I see that there are people and families who lack awareness; if they have a daughter with a disability, they hide her from people. She is not seen, no one sees her or knows about her; they are ashamed of her, especially the girls; they do not let anyone see her.” (P18).
Preferences
Participants emphasized the critical importance of privacy and gender sensitivity in healthcare. One participant preferred female healthcare providers for her daughter, reflecting cultural norms that prioritize gender concordance in medical interactions. Another participant recounted her preference for receiving care in a private room to protect her dignity after a visible amputation, underscoring the psychological and social impacts of physical vulnerability.
“She is a girl; it’s good for her to have a female doctor, not a male doctor. Now, my daughter is young, but with older girls, they prefer a female doctor; there should be a choice. Society prefers female doctors more than male doctors.” (P17).
“When I would go to the hospital, I would ask the doctor to provide private room for myself. I did not want to deal with people’s stares or their questions. I would be there for a surgery or a cesarean birth, feeling exhausted, and they would ask why there’s no leg, why a leg is being removed. It is something new to them, the first time they’re seeing such a scene. The questions are very bothersome. I would request to be alone, not wanting anyone else in the room with me.” (P18).
Safety concerns for women with disabilities
One father expressed specific protection concerns for his girl with physical disability, highlighting how this affects girls more than boys. He fears that boys or men might say something to her that is why he feels she needs protection.
“From my point of view, there’s no difference between boys and girls in regard to accessing healthcare services. However, the main issue is that because she is a girl, she requires more attention, and I feel obligated to accompany her to healthcare services. I believe that, as a girl, she is vulnerable and unable to defend herself if needed. I worry that boys or men might say something inappropriate to her, which is why I think she needs protection.” (P13).
Discrimination by nationality
Although all nationalities have been affected by the economic crisis and currency depreciation in Lebanon, Syrians and Palestinians had better access to healthcare than Lebanese because most were already registered in UN & NGOs prior to the crisis and had benefited from NGO programs that target these nationalities specifically. However, two participants suggested that Syrian nationals are more prone to discrimination.
“First, my husband is Syrian, and you’ve seen here the racism in Lebanon and the conditions and circumstances. In addition, the kids they have special needs, and they are two with the same condition that’s why it was hard for us to access healthcare services.” (P1).
Accommodation and ability to reach
Location of healthcare services and transportation
Most participants, independent of their nationality and age, complained that the locations of health care facilities are far from their home, perceiving them as “hard to reach”. Such difficulty was perceived as further exacerbated by the costs of transportation, which led many participants to walk to avoid transportation fees, which in turn exacerbated physical pain and discomfort.
“It is truly far, I am in Akkar and all the physicians and centers I access are in Beirut, I find it difficult to go there because I need to go for several rides, so the main challenge is financial where the ride to reach healthcare facility costs a lot currently” (P10).
“Most important is now the cost of transportation; if I need to go to the center, I need to pay 150,000 LL, so I decided to walk instead of paying for transportation” (P13).
Accommodation
Some participants reported that health care facilities are not accessible for persons with disabilities due to their geographical location and infrastructural barriers.
“I once took her to a center in Khalda where they offered 10 physiotherapy sessions, but she only took 6 because they had stairs and she felt tired of reaching the center” (P8).
Girls are mainly carried by their parents and brothers; in other cases, they may need healthcare assistance, such as ambulances or nurses, while those who cannot find any support report struggling to leave their houses.
She has a front and back walker but is no longer using them, because I am unable to hold her and carry the two walkers; we tried to get out of the house a few times, but she fell and hurt herself. Her father told me not to go out anymore without assistance, and our house is on the fourth floor and there is no elevator.
This barrier is not faced in ICRC-supported facilities, where physical barriers are removed as per organizational standards.
“My mother can move in her wheelchair in the facility to access care.” (p2).
Affordability and the ability to pay
Pay ability
“My husband is an employee in the municipality where they used to cover invoices, tests, and consultations. Honestly these days we are not seeking medical care of any kind even if we need it due to the financial situation, as you know the salary can barely reach 2 million LL… I am aware about the importance of monitoring my health but life hits hard, all we can do is ask about our condition, but we can’t do more” (P6).
“We are waiting for financial assistance to do surgery asap because the treatment has ended… if the money is not collected, 70% we are not going to do it” (P1).
Some participants reported having decreased the frequency of attendance at physiotherapy sessions as a result of their financial hardship.
“I have to do one physiotherapy session per week, but now I am doing it frequently depending on the financial situation, sometimes once every week sometimes once every 6 months” (p5).
Syrians and Palestinians also expressed being confronted with difficult choices when exploring their options to access health care:
“I had to do the hip surgery in Syria and come back because the UN did not cover it” (P10).
Appropriateness and ability to engage
Quality of services
The respondents’ perceptions of the quality of service received varied greatly, with several participants expressing satisfaction with the treatment received and others describing a lack of continuity of care and poor follow-up.
“All I saw were excellent services in the PHCs and at the ones I visit near my house are very organized and have a filing system for everything.” (p11).
“After the KAFO was small, no more services were provided within the organization, so they couldn’t change them. There was no proper continuity in the long term”.
Adequacy of healthcare services
Many interviewees reported that services received at the primary level of care were not sufficiently specialized for their specific needs; in particular, they could not address the rehabilitative care related to their disability.
“I need a specialized doctor in the PHC, I would have access to a family medicine doctor who will provide general prescribed medication, I won’t get proper diagnosis, I want detailed counseling and consultation on all conditions, which is not provided in the PHC” (P14).
Coordination and continuity of the services
Many women reported concerns related to the continuity of services provided at the PHCs. Participants who received their initial devices from ICRC PRP services could not afford to buy new devices when they outgrew them for both women and girls with disabilities; therefore, they have tried to do frequent maintenance rather than replacing the device with a new one as an adaptive mechanism:
“I have been using this prosthesis for 10 years and trying to do frequent maintenance; if it wasn’t for the current financial situation, I would have renewed it” (p5).
A recurrent issue identified was the lack of follow-up from their healthcare providers or the healthcare facilities that they visited, and the absence of feedback mechanisms given to them.
Interpersonal relationships between healthcare providers and patients
Participants’ experiences with healthcare providers revealed a complex interplay between respectful treatment and challenges in communication and system navigation. Many participants described positive interactions, highlighting the importance of being treated with dignity and respect during healthcare encounters. “Nobody treated us badly, nor did anyone uphold our dignity. In contrast, they were very human”. (P1)
However, not all participants shared this positive perspective. Two individuals expressed dissatisfaction with their physicians’ communication, specifically citing a lack of clear and comprehensive explanations about their daughters’ conditions.
“I needed prostheses, so I tried to go to (name of institution), but I did not find any response. Instead, I encountered rude talk and awful behavior. Honestly, I preferred to take a loan and pay for the treatment rather than being humiliated like this.” (P5).
Many participants reported a lack of possibility of directly contacting providers and a lack of coordination among different service providers, which generated difficulties in navigating the system to access the most adequate services.
Policy and legal barriers
Governmental issues
Lebanese participants understood the importance of having a disability card in facilitating their reach to healthcare centers; however, they also acknowledged limitations in the possibilities offered by it due to the financial hardship that national institutions are facing and the inequitable distribution of these disability cards.
“I didn’t get a disability card as no cards are offered now due to the economic crisis, however, sometimes people who don’t need it get it.” (P4).
Unethical behavior remains unpunished
One interesting case involving unethical behavior by a medical doctor was reported by a caregiver for a girl with disabilities. The doctor initially promised medical coverage for the girl but then disappeared, leaving the family in the difficult situation of not knowing how to cover the remaining amount. This disruption severely impacted the girl’s continuity of care, especially since they could no longer contact the doctor for advice on her condition, which required continued monitoring. The family remains uncertain where there are no legal rights to protect them.
Participants’ suggestions
The study participants formulated several suggestions, among which the most recurrent ones were related to the need to integrate affordable and specialized medical services at PHCs, and guarantee financial support and transportation allowances. Other suggestions included improving the availability of information about services available through public channels, establishing local medical centers to reduce transportation barriers, integrating rehabilitative care among primary health care services, removing physical and environmental barriers in healthcare facilities, improving the frequency of monitoring and follow-up for those who use devices over a long time, and planning for continuity of care plans for service users who benefit from devices from initiatives when these services stop.
Discussion
Women and girls with disabilities often have very specific rehabilitative and health access needs, especially in the context of conflict and violence. However, there is limited evidence on how these are being incorporated into rehabilitation program design in humanitarian settings [17]. Our study contributes valuable insight into how humanitarian rehabilitation programs can better address the intersecting vulnerabilities determined by gender and disability, suggesting potential venues to strengthen inclusive approaches emerging from the lived experience and unique stories and emotions of women and girls with disabilities in Lebanon. In fact, while the quantitative component of this mixed-methods study confirms how women and girls with disabilities still constitute only a marginal proportion of service users, its qualitative component sheds light on the reasons behind their constrained access to health care services, identifying the compounding challenges that affect their health-seeking behaviors and raising their voices to suggest potential solutions.
The underrepresentation of women and girls accessing physical rehabilitation services in Lebanon, while contrasting sharply with global estimates [1], is consistent with findings across different humanitarian settings [4, 18]. Despite evidence suggesting that early integration of rehabilitation in crises is beneficial for improving patient outcomes and despite the latest recommendations in this regard from the World Health Organization’s Emergency Medical Teams initiative [19], this specific component of care has traditionally been overlooked [20]. When integrated into the humanitarian health response, the focus of rehabilitation has typically been on trauma care and orthopedic surgery [17]. However, how rehabilitative needs for women and girls might encompass different health domains and require addressing long-term gynecological and psychological disabling consequences triggered by conditions other than trauma, such as conflict-related sexual violence, has recently been highlighted [21].
One exception to these general patterns was detected among Palestinian girls and young women. Although slight variations may not indicate significant gender disparities due to the small sample size within specific age ranges or the nature of the services provided, we can still reflect on such observations. One possible explanation for such differences lies in the structural environment in which Palestinians live in Lebanon, combined with the specific focus of some NGOs. In fact, unlike Syrian refugees who are under a non-encampment policy, almost half of the Palestinian refugees in Lebanon reside in 12 formal refugee camps [22, 23]. The United Nations Relief and Works Agency for Palestine Refugees in the Near East (UNRWA) also recently formed an agreement with the Palestine Red Crescent Society (PRCS) to provide equitable access secondary to health care services for Palestinian refugees in these camps, including through the Palestinian Disability Forum Center [22, 24]. The availability of these services inside the camps suggests that proximity of services to people in need might help overcome commonly reported barriers to accessing health care among women with disabilities, such as transportation costs, security and safety reasons, lack of information on available services, and accommodation [11]. Additionally, the UNRWA has developed a plan to ensure that its services and opportunities are more accessible to persons with disabilities by identifying and removing any physical barriers on their premises and among the youth specifically, in addition to increased screening in newborns to identify children with disabilities who might require regular treatments and additional health care support, including referrals [25]. All these enablers may have facilitated access to healthcare services for Palestinian women and girls with disabilities.
There are some elements emerging from our quantitative analysis that might partly explain the predominance of male service users in physical rehabilitation services, in addition to the hypothesized easier access to services. In fact, amputation emerges as the predominant reason for utilizing rehabilitation services within ICRC programs. This might be attributed to the contextual burden of traffic incidents, poor diabetes control, and insufficient health promotion for diabetes prevention and management [26, 27]. These underlying factors are exacerbated by the progressive weakening of the Lebanese health system, coupled with an increase in injuries resulting from war, particularly among male refugees [28]. Another study conducted in Lebanon investigated the causes behind disability amputations, and similar to our findings, more men than women underwent amputations in Lebanon, with amputation caused by poorly controlled diabetes showing a preponderance [29].
While many of the reported barriers to accessing rehabilitative healthcare are common to both men and women with disabilities, there are unique challenges that specifically affect women and girls that emerged through our interviews. A lack of information on available services, health literacy, geographical distance, financial constraints, and inadequate accommodations are examples of barriers that affect persons with disabilities of all genders. On the other hand, societal norms, in the context of Lebanon and more generally in the Middle Eastern region, place women in a heightened vulnerable state. Participants suggested that women and girls have less autonomy than men and boys in seeking care, which exacerbates their invisibility and marginalization within the community. The intersectional amplifying effects of gender, disability, and nationality were also identified in a recent report analyzing the obstacles encountered by women and girls when accessing humanitarian organizations in Lebanon. This report states that beyond the difficulties experienced by all vulnerable communities in the country, women and girls encounter further barriers linked to their gender. These include restricted access to public spaces due to traditional gender norms and roles and fewer social interactions, limiting access to information on services, which is crucial in accessing humanitarian aid. Finally, intersectional barriers, including nationality, immigration status, and/or sexual orientation, can further exacerbate access challenges [30]. Additionally, this report claims that humanitarian service providers themselves fall short of being fully equipped to reach and respond to the needs of women and girls in a tailored manner. Moreover, limited analysis of gender inclusive data and weak gender sensitive humanitarian approaches to program planning can exacerbate the gap in meeting this population’s needs. These include hidden issues such as women not being able to be physically present in public places and their limited ability to dedicate time to certain humanitarian activities because their roles in the household can further increase the gap in meeting the needs of this population [30].
Safety concerns are also an issue for women and girls with disabilities when traveling long distances to access healthcare services, who, as perceived by their caregivers, need protection when they leave the house from discrimination and harassment in society. This finding is also in agreement with results from a 2022 report on The Status of Women with Disabilities in Lebanon, which expressed similar challenges [11]. Additionally, even though participants did not identify any gender discrimination issues in the healthcare institutions they visited, having female healthcare providers attend to them is favored. Discrimination was, however, experienced among Syrian participants, who, due to the situation in the country, face different treatments in the healthcare facilities that they visit, among other settings in the country.
The financial burden of healthcare expenses may disproportionately affect women due to existing gender disparities in employment and income. Limited access to stable employment and financial resources further constrains women’s ability to afford necessary medical treatments or transportation costs. In addition, inadequate accommodations in healthcare facilities have unique implications for women’s health and dignity. Issues such as inaccessible restroom facilities or the absence of privacy measures disproportionately impact women, leading to discomfort, embarrassment, or feelings of exclusion [31, 32]. Furthermore, gender-specific healthcare needs, such as reproductive health services or maternal care, may not be adequately addressed for women with disabilities. This was also the case for one participant who preferred to be isolated from other women during pregnancy delivery to avoid judgment and discrimination from other people in the hospital. The lack of specialized care tailored to women’s health needs contributes to disparities in health outcomes and delays in seeking healthcare.
The findings regarding the appropriateness of healthcare services for women and girls with disabilities reveal several critical issues that impact their overall access to and experience with healthcare in Lebanon. While some participants expressed satisfaction with certain aspects of healthcare services, such as physiotherapy, there were significant concerns about the overall quality and continuity of care. Many participants highlighted the inadequacy of primary healthcare services in addressing their specialized needs related to disability, such as the lack of specialized treatments and counseling at PHCs. Additionally, challenges related to the coordination and continuity of services, particularly in terms of access to ongoing physiotherapy or prosthetic adjustments, were reported, often due to financial constraints and non-sustainable funding. The lack of follow-up and feedback mechanisms from healthcare providers further exacerbates these issues, leading to feelings of uncertainty and dissatisfaction among participants.
Strengths and limitations
This study had several noteworthy strengths that significantly enhanced its contribution to the literature. Although not the first such study in this field, our study uses a qualitative approach to explore healthcare barriers for women and girls with disabilities in Lebanon. In contrast to a prior report with a primarily quantitative focus [11], our research employs in-depth qualitative methods, offering richer insights into the challenges faced by this group. This, combined with a diverse and large sample for analysis, enhances the depth and breadth of our understanding of the identified barriers. In addition, the consistency of our findings with prior research conducted in humanitarian settings in general and in Lebanon in particular further strengthens the robustness of our results.
Some limitations are worth mentioning. First, the design of the ICRC program and its support criteria restricted our ability to capturing the experiences of women and girls with physical disabilities exclusively. While our findings provide valuable insights into this specific subgroup, it is important to recognize that there are diverse forms of disability, and the experiences of our sample may not be representative of those faced by women and girls with cognitive or sensory disabilities. This limitation underscores the need for future research endeavours that encompass a broader spectrum of disabilities to ensure a more comprehensive understanding of the challenges encountered by women and girls with varying disability types. Moreover, our study exclusively included women and girls with disabilities, which allowed for an in-depth exploration of barriers specific to this population. While some challenges highlighted in this study were closely linked to cultural and gender roles unique to this population, other challenges mentioned have previously been reported by both men and women. Future research should distinguish between gender-specific and shared challenges to provide a more comprehensive understanding of healthcare access barriers. Social desirability bias could have influenced the responses provided by women, girls, and their caregivers, potentially leading to skewed or idealized accounts of their experiences. Furthermore, our reliance on convenience sampling methods and the PRP database for participant recruitment might have introduced selection bias, impacting the representativeness of our sample. The individuals interviewed might represent those who are more proactive in seeking healthcare, potentially excluding those facing the most significant barriers, leading to an incomplete representation of the disability population in Lebanon. Another limitation could be identified in our study’s geographic scope, as the challenges faced by women and girls with disabilities might vary across different regions and nationalities. Finally, the ever-evolving nature of healthcare policies and social contexts introduces a temporal limitation to our findings, as the identified barriers might change over time.
While our study provides a foundational understanding, it serves as a preliminary exploration. Future investigations into the healthcare needs and access barriers of persons with physical disabilities in Lebanon must adopt a more comprehensive approach. This should involve targeting persons with disabilities from diverse regions across Lebanon across different geographical areas, ensuring a more inclusive representation.
Recommendations for future program design and implementation
In light of the findings of our study, in the context of the broader literature on disability and gender in humanitarian settings and considering the increased burden of disability that the ongoing conflict in Lebanon is expected to generate, we recommend some strategic adaptations for humanitarian health programs to promote gender equitable and disability inclusive service delivery models to ensure better health outcomes for this vulnerable population.
Integrating rehabilitative care across the continuum of patient-centered care
Disability-inclusive and gender-sensitive care needs to be integrated at all levels of health interventions, from communities to health facilities. Relevant information about healthcare services and facilities should be readily available and accessible to women and girls with disabilities. Healthcare institutions, NGOs, and local authorities should develop inclusive communication strategies using formats and channels to ensure that individuals, regardless of their ability status and area of residence, have equal access to health information. This includes information on the available services, when and where they are being provided, and who is eligible to receive them [33]. Integrating affordable medical services and quality medications into PHCs can enhance accessibility and reduce the financial burden on the most vulnerable groups in a community, particularly women and girls with disabilities. Expanding specialized services within PHCs to meet diverse healthcare needs can also reduce the need for individuals to travel to distant centers for specific services, improving access and convenience [34]. Particular attention should be given to improving access to sexual and reproductive health services and to using these services as entry points for inclusive and holistic promotive, preventative, curative, and rehabilitative care [35,36,37]. Additionally, investing in capacity building for the healthcare workforce in pediatric- and obstetric-related disability rehabilitation is crucial for addressing the specific needs of this population and improving overall access to care [38].
Strengthening intersectional approaches in humanitarian health care programming
Enhancing humanitarian actors’ understanding of the existing barriers to accessing humanitarian services for different vulnerable groups is essential for adopting relevant and targeted strategies and programs. A deeper understanding requires better data, disaggregated at least by age, gender, and ability status, to identify how these different factors intersect differently in different contexts [39]. Through such improved analysis, humanitarian organizations can develop gender-sensitive and disability-inclusive approaches to improve program design for the most vulnerable and at-risk populations, with women and girls with disabilities representing a group facing intersecting challenges in accessing essential services.
Improving culturally congruent humanitarian health programming [40]
Implementing disability-inclusive and gender-responsive programming involves tailoring healthcare services to meet the specific needs and preferences of women and girls with disabilities in specific settings. Examples from global programs include having female healthcare providers deliver care and services to enhance comfort and trust among female patients, especially for those with disabilities who prefer to be given extra privacy from others during care. The training and retention of female rehabilitation workers should be increased, particularly in contexts where the gender of the provider might influence care seeking, expanding capacity-building efforts for the healthcare workforce in pediatric and obstetric disability rehabilitation [41].
Promoting patient empowerment and meaningful engagement
In-service delivery participatory design approaches are essential for ensuring that healthcare programs effectively meet the needs and preferences of women and girls with disabilities. While securing organizational buy-in and funding for these adaptations may require advocacy and resource mobilization, highlighting the potential impact on improving healthcare access and outcomes for women and girls with disabilities can help garner support and prioritize these initiatives [42]. Tailored cash-based interventions or income-generating activities to support the financial independence of women with disabilities might further empower this vulnerable group, allowing for more flexibility in seeking care and avoiding reliance and dependence on caretakers [43, 44], as well as reducing the risk of negative coping mechanisms [45]. The implementation of educational programs aimed at raising awareness among women with disabilities and their families can help prevent social exclusion, provide social support, and foster positive attitudes toward healthcare-seeking behavior. Such initiatives can significantly benefit from involving men and male authority figures to enable better access for women and girls with disabilities, especially in sexual and reproductive health (SRH) and sexual and gender-based violence (SGBV) initiatives [46, 47]. This approach aligns with WHO recommendations on engaging men as allies in promoting women’s human rights, with the potential for transformative change in humanitarian settings [48].
Conclusion
Women and girls with disabilities are affected by intersecting vulnerabilities that can constrain their access to healthcare services in general and rehabilitative services in particular. A more inclusive and culturally sensitive rehabilitation program design, a specialized training program for the rehabilitation workforce, and improved humanitarian policies could help overcome some of these barriers. In particular, we recommend expanding admission criteria to include causes of disabilities other than trauma-related ones, which might disproportionately affect women and girls; increasing the training and retention of female rehabilitation workers, particularly in contexts where the gender of the provider might influence care seeking; expanding capacity-building efforts for the healthcare workforce in pediatrics- and obstetrics-related disability rehabilitation; and integrating rehabilitation services at the primary level of care. While further research is needed to shed light on what will work in the long term, focusing on the abovementioned points can critically support improving access to rehabilitative care for women and girls with disabilities in the short to medium term, potentially avoiding further complications and contributing to advancing gender equity. This becomes particularly urgent with the increasing number of people wounded in Lebanon, that might increase the burden of unmet rehabilitative needs across all segments of the population.
Data availability
No datasets were generated or analysed during the current study.
Abbreviations
- ICRC:
-
International Committee of the Red Cross
- PRP:
-
Physical rehabilitation program
- LMICs:
-
Low-and-middle-income countries
- MOSA:
-
Ministry of Social Affairs
- PHC:
-
Primary Healthcare
- NGOs:
-
Non-Governmental organizations
- UN:
-
United Nation
- UNRWA:
-
United Nations Relief and Works Agency for Palestine Refugees in the Near East
- KAFO :
-
Knee Ankle Foot Orthosis
References
United Nation (UN), making the SDGs count for women and girls with disabilities. New York: UN Women; 2017.
Matin BK, et al. Barriers in access to healthcare for women with disabilities: a systematic review in qualitative studies. BMC Womens Health. 2021;21(1):44.
Jolof L, et al. Experiences of armed conflicts and forced migration among women from countries in the Middle East, Balkans, and Africa: a systematic review of qualitative studies. Confl Health. 2022;16(1):46.
United, Nations. Convention on the rights of persons with disabilities. Eur J Health law. 2007;14(3):281–98.
Barth CA, et al. Users of rehabilitation services in 14 countries and territories affected by conflict, 1988–2018. Bull World Health Organ. 2020;98(9):599.
McPherson A, et al. Strengthening health information systems for disability-related rehabilitation in LMICs. Health Policy Plann. 2016;32(3):384–94.
World Bank country and lending groups. https://datahelpdesk.worldbank.org/knowledgebase/articles/906519-world-bank-country-and-lending-groups. Accessed 29 Jan 2024.
El Sayed MJ. Beirut ammonium nitrate explosion: a man-made disaster in times of the COVID-19 pandemic. Disaster Med Pub Health Prep. 2022;16(3):1203–7.
Rigby SE, et al. Preliminary yield estimation of the 2020 Beirut explosion using video footage from social media. Shock Waves. 2020;30(6):671–5.
Ministry of Public Health (MOPH). https://www.moph.gov.lb/userfiles/images/Prevention/PHEOC/Cumulative%20Report%20on%20the%20Total%20Number%20of%20Martyrs%20and%20Wounded%20since%20the%20Start%20of%20the%20Aggression/24-11-2024-2-eng.jpg. Accessed 25 Nov 2024.
Feghali J. The status of women with disabilities in Lebanon: a snapshot of socio-political and economic impacts from an intersectional lens. The International Foundation for Electoral Systems, ABAAD, and the Lebanese Union for People with Physical Disabilities. Lebanon. 2022. https://www.ifes.org/sites/default/files/migrate/status_of_women_with_disabilities_in_lebanon_accessible.pdf.
Multi-sectoral needs assessment (MSNA) Lebanon 2021 disaggregated data report: gender, age, disability. 2022. https://lebanon.unwomen.org/sites/default/files/2022-05/MSNA%20-%20disaggregated%20data%20report%20-%20gender%2C%20age%2C%20disability%20_%20FINAL%202021.pdf.
UNHCR. Lebanon inter-agency coordination - in focus: women, girls, men and boys with disabilities in Lebanon. In: The impact of Lebanon’s crisis on persons with disabilities: protection risks, cross-sectoral response and recommendations. 2023. https://reliefweb.int/report/lebanon/lebanon-inter-agency-coordination-focus-women-girls-men-and-boys-disabilities-lebanon. Accessed 6 Jan 2024.
Chaiban L, et al. Access to primary and secondary health care services for people living with diabetes and lower-limb amputation during the COVID-19 pandemic in Lebanon: a qualitative study. BMC Health Serv Res. 2022;22(1):593.
Levesque J-F, Harris MF, Russell G. Patient-centred access to health care: conceptualising access at the interface of health systems and populations. Int J Equity Health. 2013;12(1): 18.
Cu A, et al. Assessing healthcare access using the Levesque’s conceptual framework– a scoping review. Int J Equity Health. 2021;20(1):116.
Jain RP, et al. Delivering trauma and rehabilitation interventions to women and children in conflict settings: a systematic review. BMJ Glob Health. 2020;5(Suppl 1): e001980.
Barth CA, et al. Retrospective observational study of characteristics of persons with amputations accessing International Committee of the Red Cross (ICRC) rehabilitation centres in five conflict and postconflict countries. BMJ open. 2021;11(12): e049533.
World Health Organization (WHO). Emergency medical team strategy 2030. 2022. https://www.who.int/news/item/04-10-2022-who-launches-the-emergency-medical-teams-2030-strategy-at-global-meeting-to-strengthen-rapid-response-amid-emergencies-worldwide.
Amatya B, Khan F. Disaster response and management: the integral role of Rehabilitation. Annals Rehabil Med. 2023;47(4):237.
Morgan R, et al. Rehabilitation services must include support for sexual and gender-based violence survivors in Ukraine and other war- and conflict-affected countries. Health Policy Plann. 2023;38(3):417–9.
Saleh S, et al. Integrating refugees into national health systems amid political and economic constraints in the EMR: approaches from Lebanon and Jordan. J Global Health. 2022;12:03008. https://doiorg.publicaciones.saludcastillayleon.es/10.7189/jogh.12.03008.
UNRWA. Where we work. UNRWA; 2023. https://www.unrwa.org/where-we-work/lebanon.
Anera. Providing support for physically disabled Palestinian refugees in Lebanon. Anera; 2018. https://www.anera.org/stories/support-disabled-palestinian-refugees-lebanon/.
UNRWA. Transforming the lives of palestine refugees with disabilities. unrwa; 2017. https://www.unrwa.org/resources/about-unrwa/transforming-lives-palestine-refugeesdisabilities.
McDonald CL, et al. Global prevalence of traumatic non-fatal limb amputation. Prosthet Orthot Int. 2021;45(2):105–14.
Barnes JA, et al. Epidemiology and risk of amputation in patients with diabetes Mellitus and Peripheral Artery Disease. Arterioscler Thromb Vasc Biol. 2020;40(8):1808–17.
Kobeissi E, et al. Long-term burden of war injuries among civilians in LMICs: case of the July 2006 war in Lebanon. Front Public Health. 2023;11:1305021.
Yaghi K, et al. Diabetes or war? Incidence of and indications for limb amputation in Lebanon, 2007. East Mediterr Health J. 2012;18(12):1178–86.
Referral information management system (RIMS), women’s barriers to access humanitarian services. https://www.referral-ims.org/wp-content/uploads/Womens-barriers-to-access-humanitarian-services.pdf.
Hejase AJ, Hejase HJ, Hejase HA. Gender wage gap in Lebanon: explorative analysis. J Appl Econ Bus Res JAEBR. 2015;5(1):1–19.
United Nations. (UN), 2022 women’s economic participation in lebanon: a mapping analysis of laws and regulations. United Nations Economic and Social Commission for Western Asia. https://www.unescwa.org/sites/default/files/pubs/pdf/women-economic-participation-lebanon-mapping-analysis-laws-english.pdf.
UNICEF. Access to humanitarian aid challenges and recommendations for women and men, girls and boys with disabilities. 2019. https://www.unicef.org/mozambique/media/2386/file/Access%20to%20humanitarian%20aid%20for%20women%20and%20men,%20girls%20and%20boys%20with%20disabilities.pdf.
Truppa C, et al. Developing an integrated model of care for vulnerable populations living with non-communicable diseases in Lebanon: an online theory of change workshop. Confl Health. 2023;17(1):35.
Tanabe M, et al. Intersecting Sexual and Reproductive Health and disability in humanitarian settings: risks, needs, and capacities of refugees with disabilities in Kenya, Nepal, and Uganda. Sex Disabil. 2015;33(4):411–27.
Scolese A, et al. Disability status and violence against women in the home in North Kivu, Democratic Republic of Congo. Glob Public Health. 2020;15(7):985–98.
Hossain M, et al. Disability, violence, and mental health among Somali refugee women in a humanitarian setting. Glob Ment Health (Camb). 2020;7:e30.
Jain RP, et al. Delivering trauma and rehabilitation interventions to women and children in conflict settings: a systematic review. BMJ Glob Health. 2020;5(Suppl 1): e001980.
UN Office for Disaster Risk Reduction. Sendai framework monitor (SFM) sex, age and disability disaggregated data (SADDD). https://wrd.unwomen.org/sites/default/files/2022-05/P2129-Sendai%20Framework%20Monitor_SADDD-digital_LR.pdf.
Khalid S, Dixon S, Vijayasingham L. The gender responsiveness of social entrepreneurship in health – a review of initiatives by Ashoka fellows. Soc Sci Med. 2022;293:114665.
Witter S, et al. The gendered health workforce: mixed methods analysis from four fragile and post-conflict contexts. Health Policy Plan. 2017;32(suppl5):v52-62.
World Health Organization. WHO framework for meaningful engagement of people living with noncommunicable diseases, and mental health and neurological conditions. 2023. https://iris.who.int/bitstream/handle/10665/367340/9789240073074-eng.pdf?sequence=1.
Thakkar K, et al. The role of cash and voucher assistance in increasing equity and inclusion for girls and children with disabilities in education in emergencies. 2023. https://inee.org/sites/default/files/resources/CVA%20in%20EiE%20girls%20%2B%20cwds%20rgb%20ONLINE%20final.pdf.
Lyles E, et al. Multi-purpose cash transfers and health among vulnerable Syrian refugees in Jordan: a prospective cohort study. PLOS Global Public Health. 2022;2(11): e0001227.
Salti N, et al. The impact of cash transfers on Syrian refugees in Lebanon: evidence from a multidimensional regression discontinuity design. J Dev Econ. 2022;155: 102803.
World Health Organization (WHO). WHO recommendations on health promotion interventions for maternal and newborn health. 2015. https://www.ncbi.nlm.nih.gov/books/NBK304983/.
Shand T, Marcell AV. Engaging men in sexual and reproductive health. In: Oxford research encyclopedia of global public health. 2021. https://oxfordre.com/publichealth/view/10.1093/acrefore/9780190632366.001.0001/acrefore-9780190632366-e-215.
UN. 9 ways men can become allies for equal rights. 2020. https://eca.unwomen.org/en/news/stories/2020/9/9-ways-men-can-become-allies-for-equal-rights.
Acknowledgements
The authors express gratitude to all the women and girls with disabilities as well as their caregivers who participated in the study. Additionally, we acknowledge the dedicated ICRC physical rehabilitation team in Lebanon for their committed efforts in data collection.
Author information
Authors and Affiliations
Contributions
CT and AB conceptualized the study idea. LAA, HR, and AM developed the proposal and prepared the interview topic guide. LAA and RR conducted the quantitative data analysis. DS, RM, and HR conducted the interviews, while DS and LAA were responsible for transcription and translation. LAA, DS, and ML analyzed the qualitative data, with contributions to qualitative data analysis from LV and CT. LAA, DS, and ML drafted the manuscript. CT, RR, LV, AB, AM, HR and HS provided assistance in editing and reviewed the article for important intellectual content. All authors approved the final version submitted.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study received ethical approval from the International Committee of the Red Cross (ICRC) ethical review board (Reference: LDP_CORE 23/00007 - CGB/bap). Participants were fully informed of their rights, including voluntary participation and the option to withdraw consent without consequences. They were also assured that their decision to participate would not affect their regular access to services. All participants provided written informed consent.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

{kind=link}
Cite this article
Abou-Abbas, L., Sabbagh, D., Rossi, R. et al. Challenges in accessing health care services for women and girls with disabilities using a humanitarian physical rehabilitation program in Lebanon: a mixed method study. Int J Equity Health 23, 267 (2024). https://doiorg.publicaciones.saludcastillayleon.es/10.1186/s12939-024-02356-4
Received:
Accepted:
Published:
DOI: https://doiorg.publicaciones.saludcastillayleon.es/10.1186/s12939-024-02356-4