- Research
- Open access
- Published:
Physical-medical integration policies and health equity promotion in China: a text analysis based on policy instruments
International Journal for Equity in Health volume 23, Article number: 266 (2024)
Abstract
Background
In China, although policies promoting physical-medical integration have received widespread national attention, the existence and manifestation of health equity promotion within these policies still require further exploration.
Methods
This study used text analysis to examine 62 policy documents on physical-medical integration issued by various Chinese governmental departments from June 2016 to June 2023, utilizing KH Coder software for qualitative analysis.
Results
The analysis revealed a strong emphasis on public health, promoting health management and disease prevention across all age groups. The policies aimed to ensure the equitable distribution of health care resources, particularly those benefiting rural and underserved populations, and they underscored the importance of collaboration among the government, sports, and health care sectors to foster sports-health integration.
Conclusion
The integration of sports and health policy is a key initiative to address chronic diseases in China, as it aligns closely with health equity principles. Achieving these goals requires ongoing improvements in implementation and monitoring, with a focus on the diverse needs of various populations.
Background
Health is not only a personal need but also a basic right of every human being [1]. Thus, health equity is one of the important goals pursued by the development of human society, and it is an important foundation for the survival and development of human society [2]. The issue of health equity has been increasingly emphasized worldwide and has become one of the focuses of health issues globally [3]. Thus, health equity has become an important guide for health policy-making [4]. In 2022, the World Health Organization (WHO) released a report titled “World Health Statistics 2022: Monitoring Health for the SDGs, Sustainable Development Goals”. The report’s statistics cover the period up to 2020, and it features updated summaries of global and regional trends in life expectancy and healthy life expectancy, the global burden of disease and injury, and major health risk factors [5].
In China, health issues are also of great concern. According to the report “World Health Statistics 2022: Monitoring Health for the SDGs, Sustainable Development Goals”, China’s life expectancy is 77.4 years (74.7 years for men and 80.5 years for women), and healthy life expectancy (HALE) is 68.5 years (67.2 years for men and 70.0 years for women). In China, 4 types of chronic diseases lead to premature death. In 2019, the probability of death from any of the 4 major non-communicable diseases (NCDs), namely, cardiovascular disease, cancer, diabetes, and chronic kidney disease, was 15.9% (nearly 1 in 6) for people aged 30 to 69 years. In addition, in terms of health risk factors, the prevalence of tobacco use among people aged 15 years and older was 25.6%; per capita, alcohol consumption among people aged 15 years and older was equivalent to 6 L of pure alcohol; the age-standardized prevalence of hypertension among adults aged 30 to 79 years was 27.3%; the age-standardized prevalence of obesity among children and adolescents (5 to 19 years) was 11.7%; and the age-standardized prevalence of obesity among adults (18 years old and older) was 6.2% [5]. Moreover, China faces the same public health equity or inequality problems. Health inequities are on the rise, and health disparities between regions and populations, as well as disparities in the accessibility of health services, have developed to the point where they must be addressed [6]. The facts above show the health inequalities that exist globally, the differences in the distribution of health care resources faced by different populations, and the impact of these inequalities on the health of society as a whole.
With China’s ageing population increasing year by year, the burden of chronic diseases has intensified, while health care inequalities have led to an urgent need for better health care and disease management [7]. In addition, because sports are characterized by body management and discipline, the sports system can effectively penetrate dietary nutrition, health management, medicine, and the health system to protect human health, safety and life, highlighting the improvement in the national governance capacity and the optimization of the means of governance [8]. Therefore, China has developed physiological-medical integration and non-medical health intervention policies to promote the national shift from passive medical treatment to active health. China has implemented an integrated health, care, and sports policy known as the sports-health integration policy. This policy aims to address the challenges of an ageing population by promoting collaboration between the sports and medical sectors, with the goals of improving public health and preventing diseases [9]. Since the 2016 Healthy China Development Outline was proposed, the physiological-medical integration policy, an innovative model for integrating sports and medical resources to achieve comprehensive health, has attracted widespread attention, with the public gradually becoming aware of it [10]. The physiological-medical integration policy can be regarded as a guiding document for the direction of health governance development in China for the foreseeable future. The relevant departments of health and sports in the Chinese government have subsequently developed several supporting policies. Specifically, physiological-medical integration is a cross-disciplinary approach between sports and medicine that aims to provide personalized health care and health management services to improve all aspects of health care and to optimize health care outcomes, resource allocation, and health experience [11].
This is the most influential policy tool in China’s health governance, and it will have the longest-lasting impact in the future. Since a series of policy texts related to China’s physiological-medical integration policy does not directly provide a reference for health equity, does this important health policy reflect health equity, how does this policy tool promote health equity, and what improvements in the physiological-medical integration policy can be realized through the lens of health equity? The integration of policy through the lens of health equity needs to be further explored. To address this issue, this paper conducts an in-depth study of physiological-medical integration policy text and health equity promotion through the text analysis tool KH Coder, with the aim of optimizing this policy and providing a theoretical basis and decision-making support for policy adjustment and optimization. This theoretical foundation and decision-making support will help China become a sports powerhouse and improve the health of the whole population.
Research design
Literature review
In the field of health policy integration, existing research has emphasized the positive impact of integration on the accessibility of health services. For example, integrating different health services can effectively enhance the efficiency of resource utilization, thereby improving public health [12]. However, studies have focused primarily on integration within a single domain, a specific exploration of cross-sector integration, such as the integration of sports and medicine, is lacking. Additionally, while research has highlighted the critical role of interdepartmental collaboration in improving the quality of health services, empirical studies on the effectiveness of policy implementation across different sectors are lacking. In particular, in the context of sports-health integration, the literature has not sufficiently examined how this integrated policy specifically impacts the health outcomes of different population groups [13]. In terms of health equity, policy-makers must focus on ensuring that all population groups, especially vulnerable groups, have equal access to health resources [14]. However, current research often overlooks issues of equity in the policy implementation process, particularly at the intersection of sports and medicine [15]. This gap highlights the importance of research in this area.
In the specific literature on sports-health integration, studies have shown that health policy integration often fails to effectively address health disparities between different groups, underscoring the importance of focusing on health equity in policy evaluation [16]. However, research has focused primarily on health care services and has not explored the potential of sports policies in promoting health equity in depth. Additionally, some studies have emphasized the importance of physical activity in disease prevention and overall health promotion [17]. Furthermore, despite the widespread discussion on the integration of sports and health policies, systematic research evaluating their actual impact on health equity is lacking.
The studies above indicate that while the literature has explored the integration of health policies and equity, there remains a significant research gap regarding the specific impacts of sports and medicine integration policies. This paper aims to fill this gap by systematically analysing the texts of sports and medicine integration policies and their effects on health equity, providing valuable insights for policy-makers.
Analytical framework
In October 2016, China introduced an important document for the integration of physical and medical policies, namely, the “Healthy China 2030” Planning Outline. Various relevant government departments subsequently developed complementary policy texts. In response to this policy, which has a significant impact on the health of Chinese citizens, this paper explores the presence and manifestations of health equity concepts within policy tools on the basis of Roswell and Walter’s three types of policy instruments (demand-based policy instruments, supply-based policy instruments, and environment-based policy instruments). To examine this topic in depth, this paper adopts an analytical framework constructed with the X policy MEANS (policy type) dimension and the Y policy ENDS (health equity) dimension.
First, we discuss the X dimension, that is, the fundamental policy instrument dimension. The existence of health equity within policy objectives and its manifestations is examined in this section. Based on the MEANS-ENDS relationship between policy tools and policy objectives and integrating theories of policy evaluation from the literature, this study closely associates health equity goals within physical-medical integration policies with the effectiveness and efficiency of policy tools. Specifically, we first analyse the MEANS-ENDS relationship between policy objectives and policy tools. Research indicates that the choice of policy tools directly affects the degree to which policy objectives are achieved, particularly in policies related to health equity, where the effectiveness and efficiency of tools are especially critical [18]. Therefore, this study focuses on assessing the means employed in physical-medical integration policies (such as strategies, measures, and tools) and correlating them with policy objectives (such as health equity, access to medical resources, and the promotion of physical activity) to analyse their effectiveness and resource utilization efficiency in advancing physical-medical integration and health equity. Additionally, based on the classification theory of policy tools in the literature, this study categorizes the tools of physical-medical integration policies into three types: demand-based policy instruments, supply-based policy tools, and environmentally based policy instruments [19]. This classification aids in further assessing the contributions of different tools to health equity objectives. Finally, this study explores the specific manifestations of health equity within policy goals. Research indicates that achieving health equity requires policies to be inclusive and to effectively reduce disparities in access to medical and physical activity services [20]. This study evaluates the effectiveness of physical-medical integration policies across different populations by examining the details of implementation, including the target groups served and the coverage of policy initiatives.
Second, we discuss the Y dimension, that is, the ENDS (health equity) dimension. This study proposes the research perspective of health equity. Health equity is a crucial goal that aims to ensure equal health opportunities and resources for all individuals; it involves creating conditions that allow everyone to attain the highest level of personal health, regardless of demographic characteristics [21]. Research points out that this concept is rooted in principles of social justice and fair equality of opportunity, emphasizing that all citizens should have access to basic health systems regardless of financial resources.
Health equity is related not only to individual health status but also to the overall health disparities within society. This study emphasizes that the ultimate goal of physical-medical integration policies is to promote health equity, ensuring that different social groups have equal access to health opportunities. Therefore, as the starting point of this research, we advance the development of health equity through policy analysis, particularly within the context of physical-medical integration policies, ensuring that everyone has the opportunity to access the necessary health resources.
Third, we discuss the analysis of the X and Y dimensional framework. This study focuses on the key elements of three types of policy texts to comprehensively understand the impact of physical-medical integration policies on health equity. First, the temporal dimension is analysed. By tracing the timeline of physical-medical integration policies, the literature indicates that the evolution of these policies and their implementation timing are critical to their overall impact, with earlier policies often influencing subsequent policies. Policy implementation is affected by dynamic social and political contexts, with temporal aspects playing a significant role in shaping outcomes [22]. By documenting the release dates of policies, the historical development of the policies and the inclusion criteria are clarified, aiding in the understanding of the relationship between policy evolution and health equity. Second, attention is paid to policy sources. The literature indicates that policy-making bodies and implementing agencies play a crucial role in the credibility and effectiveness of policy enforcement [23]. By identifying the sources of policies, including government agencies, regulatory documents, or the bodies responsible for policy formulation, the authority of the policies and the responsibilities of their implementing agencies can be revealed, allowing for an assessment of their actual impact on health equity. Finally, the analysis focuses on policy themes. Research indicates that the core objectives, areas of concern, and contents of policy texts directly determine their scope and purpose of implementation [24]. Therefore, this study analyses the themes within policy texts to identify the core objectives, areas of concern, and contents of the policies, thereby clarifying the scope of implementation and the potential impact of the policies on health equity (Fig. 1).

Analytical framework
Through this analytical framework, we aim to delve deeper into the impact of body-medicine integration policies on health equity, providing policy-makers and researchers with important insights into how policy instruments shape health equity, which can help guide future policy-making and health equity promotion interventions.
Text analysis
Text analysis is a data analysis technique designed to extract meaningful information and insights from textual data [25]. Text can be any form of written or verbal expression, such as articles, emails, social media posts, comments, news reports, blog posts, and questionnaires. Text analysis usually includes the following steps. First, text data are collected. Text data from different sources are collected in one location. The second step is pre-processing. The text data are cleaned, e.g., useless characters, punctuation marks, and stop words are removed, and the text is converted into a uniform format. The third step is analysis. Different techniques and methods, such as word frequency statistics, topic modelling, sentiment analysis, and entity recognition, are applied to extract meaningful information and insights from the text. The fourth step is visualization, where the results of text analysis are visualized for better understanding and communication.
The specific methods used in this study include the following analysis methods. First, word frequency analysis is conducted. Word frequency analysis is a versatile tool in linguistic research, offering profound insights into the dynamics and evolution of language and enabling the identification of varying patterns of word usage frequency over time [26]. Word frequency analysis (WFA) is used to identify the keywords that appeared most frequently in the policy text to identify key themes and words related to health equity. Second, multi-dimensional scaling analysis is performed. Multi-dimensional scaling and correspondence analysis can uncover hidden interests and priorities in the policy-making process, offering new insights into how policies impact health equity [27]. These methods help identify patterns and trends within policy texts and evaluate the effectiveness of policies in promoting health equity. Multi-dimensional scaling analysis (MDS) is used to compare different dimensions (e.g., time, policy sources, and themes) of policy texts to identify relevance and trends. Third, correspondence analysis is conducted. Correspondence analysis (CA) is a versatile statistical technique for visualizing the associations between variables in contingency tables, where proximity represents association strength [28]. Text data on physical health integration policies are compared with concepts and indicators of health equity to assess the potential impact on health equity and the association of physical health integration policies with health equity.
Data sources and identification criteria for policy literature
Policy texts are the direct object of policy analysis; i.e., policy texts are an important data source for policy analysis. Policy texts refer to relevant laws, rules, and regulations that are usually expressed in the form of documents enacted by the state [5]. That is, a policy text is a document or collection of documents developed by a government, political party, or other political organization to prescribe or guide a particular action or policy. These documents may include official documents, policy documents, legal documents, treaties, directives, circulars, decisions, and reports. Policy texts usually reflect the objectives, philosophies, and policy directions of a government or political organization, and they serve as important guides for the public and other relevant organizations. Policy texts can be public or non-public, depending on the nature and purpose of the policy. Policy text documents used as metadata for analysis have relatively rich identifiers, through which the source, level, subject, and keywords of the policy documents can be effectively determined (Table 1).
Criteria for the inclusion of policy texts
The sources of information for this study mainly included Beida Fabo, the National Government Information Network and the website of the National Health Commission. Keywords such as sports, medical care, chronic diseases, emergencies, integration of sports and medicine, health for all and integration of sports and medicine were used to search the data. To ensure the relevance and validity of the study, the collected policy texts were screened. The following criteria were followed in the process of including policy texts. First, the included policy texts had to be released after the strategic plan of the Fifth Plenary Session of the 18th CPC Central Committee and the State Council on October 25, 2016, and had to be related to the “Healthy China 2030” Planning Outline. The timeline ends on June 30, 2023. Second, relevant documents issued by local governments were not included. Third, the content of the policy text had to be closely related to the work of physical and medical integration. Fourth, the policy texts had to be normative documents, such as outlines, plans, opinions, notices, and laws and regulations, and they had to have an issue number.
In the screening process, non-normative documents such as speeches of leaders, letters, and approvals, as well as policy documents with weak relevance to the topic of the integration of health care, were excluded. After the screening process, a total of 62 planning and policy documents on the integration of physical medicine issued at the national level in China were used as the main data source for this study (Table 2). According to Rothwell and Zegveld’s classification of supply-based, environment-based, and demand-based policy instruments [29], the classification of the 62 policy documents can be used to analyse and explore China’s national-level policies on the integration of physical medicine and to provide a scientific basis and effective suggestions for policy optimization.
Analysis tools
In this paper, KH Coder text data mining software is used to find hidden problems and assumptions by analysing specific text information. In this regard, keyword frequency analysis can reflect the degree of attention of policy-makers to each part of the content. The basis of word frequency analysis, co-occurrence network analysis, multi-dimensional scale analysis, and correspondence analysis can further reveal the theme and main idea of the policy text and then form the relevant dimensions of the research framework according to the policy content to comprehensively understand the relevant dimensions of the formulation of the policy of the integration of physical and medical care and to discover the strengths and shortcomings of the policy to provide a scientific basis for further optimization and improvement of the policy of the integration of physical and medical care. Therefore, this study selects planning policy texts, constructs a sample library of policy texts, and numbers the planning policy texts to complete the text collection and pre-processing process. On this basis, the text mining tool KH Coder software is used to analyse the policy texts.
Results
Pre-processing of the text of the policy on the integration of physical and medical care
After searching and screening, a total of 62 documents were collected. The contents of the files were co-imported into an Excel file for use in the KH Coder analysis.
After preliminary text processing by KH Coder, the total number of words in the main Excel document was 158,622 (using 110356), and the number of dissimilar words was 7645 (using 6878); the document had a fixed amount of text, which could be used to carry out text data mining by KH Coder (Table 3).
Keyword extraction and analysis
Through the text mining tool KH Coder software, the text database of the medical integration policy is divided into words and word frequency statistics, and a list of word frequencies of the characteristic words of the medical integration policy at the national level is obtained, as is the corresponding word frequency number. The high-frequency words represent the formulation goals of the national-level body-health integration policy. To reduce interference, some of the words that are meaningless to the analysis are uniformly deleted in the high-frequency word counting, such as to be, committee, new, country, China, and relevant. Additionally, terms that are not directly related to health equity, such as state and relevant, were removed from the policy texts to ensure greater precision in the analysis. The results are as follows (Table 4).
Plotting the word frequencies above shows that the circles on the curve represent the number of occurrences, with being closer to the y-axis representing more occurrences and being closer to the x-axis representing approximately fewer occurrences (Fig. 2).
Word frequency distribution
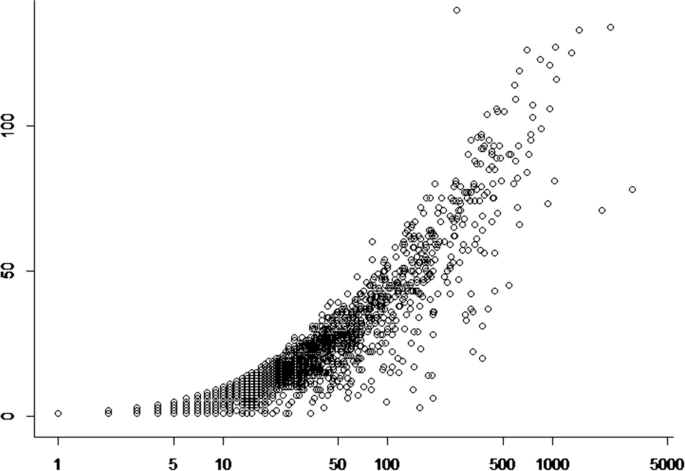
In addition, to understand whether the number of occurrences of each word is average or not, the number of occurrences of high-frequency words (TF value) and the frequency were used as two variables for curve fitting, which was found to be the closest to the power function distribution. Figure 3 shows that the distribution of high-frequency words has a clear long-tailed distribution, which is the result of the number of occurrences and the number of documents. The interpretation is similar to that in the figure above, which is in line with the obvious Matthew effect, indicating that the data obtained in this study have a better representation.

Distribution of word frequency fit
As a result, the word frequency analysis yields the following results. First, regarding health-related words, in the word frequency data, “health” is the most frequent keyword, appearing 2,758 times, indicating that the policy attaches importance to health issues. Meanwhile, health-related words such as “medical”, “hygiene” and “nutrition” also appear with high frequency, indicating the policy’s demand for and attention to health care and health care. Second, regarding macro policies and institutions, in the word frequency data, words such as “promote”, “promote” and “development” appear with high frequency, reflecting the pursuit of social development and progress. In addition, words such as “organization”, “department” and “government” highlight the important role of government agencies in promoting various activities. Third, regarding community and grassroots services, words such as “community” and “grassroots” also receive some attention in the word frequency data, indicating that focusing on grassroots services and community building has become an important goal in the field of social services. Fourth, comprehensive development is emphasized. The high frequency of terms such as “comprehensive”, “all people” and “all-round” reflects the importance of integrated development and the participation of all people. Fifth, regarding technology and information, as society continues to progress, the frequency of terms such as “technology” and “information” is high, demonstrating the important role of science, technology and informationization in various fields.
The high-frequency words above reflect the main objectives of policy formulation. In the X-axis dimension, policy tools are categorized into demand-based, supply-based, and environment-based tools. Analysis of these high-frequency words reveals that national policies predominantly employ supply-based tools, as evidenced by the frequent occurrence of terms such as “health services,” “institutions,” and “management,” which indicates the government’s focus on advancing the provision of medical services. Additionally, demand-based tools are evident in the policies, with words such as “promote,” “support,” and “implement”, suggesting that the policies aim to respond to the growing societal demand for health. Furthermore, environment-based tools are less mentioned, implying that there is less emphasis on improving the external environment in the policies.
In the Y-axis dimension of health equity, high-frequency words such as “universal,” “grassroots,” and “community” indicate that policy documents emphasize promoting health equity among different groups through the integration of medical services and physical activities. However, further analysis reveals that policies tend to focus more on specific groups (such as elderly individuals and patients with chronic diseases) while paying less attention to younger populations, indicating some deficiencies in achieving health equity.
Through the selection and cluster analysis of high-frequency words, it can be seen that the national-level sports and medicine integration policy mainly concentrates on supply-based policy tools and shows concern for promoting universal health equity. However, there are still shortcomings in terms of specific measures and implementation pathways.
Co-occurrence network analysis
Through the function of KH Coder’s co-occurrence network (the lowest word frequency is set to 15), it can be seen that the sports-medicine integration policy shown in Fig. 4 is the theme. This figure is a covariance network diagram, and it can be seen from the diagram that health, all people, hygiene, sports, physical education, and medical care are the keywords with the most co-occurrences. This once again proves that local governments in China are more concerned with the integration of sports in the formulation of sports integration policies and that the way to promote the health of the whole population is through the integration of sports and medical care. Closer to the high-frequency word health are the words service, construction, and management, which suggests that the national government is more concerned with the government-led construction of relevant service models to promote health when formulating policies for the integration of sports and medicine. Another high-frequency word, sports, is surrounded by the words fitness, all people, and exercise, which indicates that when the national government formulates policies on the integration of sports and medicine, it is clear that the prerequisite for realizing the health of all people is to do so through sports; that is, the work of realizing health is done in the ordinary course of life. In other words, the way to realize health is through physical activity. At the same time, data, medical, information, and platforms form an independent system, indicating that big data intelligent systems have gradually become a means of realizing the integration of sports and medicine.

Co-occurrence network of policies on the integration of physical medicine at the national level
Through KH Coder’s thematic co-linear relational network analysis, it is evident that policy-makers prioritize demand-based policy instruments, particularly emphasizing broad objectives such as the realization of health for all. This reflects a strong demand-side focus, where the dominant direction of the policy aligns with public health needs. However, the analysis reveals that while these policies stress the ultimate goal of health equity (Y-axis), they often lack supply-based measures that address specific interventions required to integrate sports and medical care in practice.
In terms of supply-based tools, there is minimal elaboration on concrete, group-oriented service programmes targeting different demographic groups. Instead, policies tend to favour certain segments of the population, such as elderly individuals, children, and citizens, with little focus on youths—highlighting a potential equity gap on the Y-axis. The lack of detailed strategies for specific groups reflects an imbalance in addressing diverse health needs, indicating that while demand is recognized, policies are not fully tailored to the varied supply-side needs required to achieve health equity.
Moreover, when examining environment-based policies, keywords such as services, medical care, human resources, elderly care, institutions, publicity, prevention and treatment, facilities, and industries suggest regional variability in implementation; this suggests that different areas employ different environmental tools to achieve health goals but without clearly assigned responsibilities for implementation or monitoring mechanisms (indicating inefficiency on the X-axis). The lack of explicit governance structures and detailed planning for personnel and resources further undermines both the effectiveness of supply-based tools and the ultimate goal of promoting health equity (Y-axis).
Therefore, while the policy framework aims to promote health equity (Y-axis), the absence of specific supply-based mechanisms and clearly defined environmental policies raises concerns about its actual impact. Policies lack the precise instruments necessary for effective implementation and monitoring, thus failing to fully realize the integration of sports and medicine for diverse populations.
Multi-dimensional scaling analysis
The results of the analysis (Fig. 5) reveal eight high-frequency word dimensions in the policy text on body-health integration, and these dimensions reflect different policy tools and pathways for achieving health equity.

Results of multi-dimensional scaling analysis
First, the health dimension corresponds to demand-based policy instruments and includes terms such as health, medical care, hygiene, sports, nutrition, disease, elderly, and chronic disease. These terms indicate the policy’s focus on promoting public health, improving medical services, enhancing hygiene, and addressing the health needs of elderly individuals and patients with chronic diseases. On the Y-axis, which represents health equity, this dimension demonstrates responsiveness to the health needs of vulnerable groups, particularly elderly individuals.
Second, the service and promotion dimension encompasses terms such as service, promote, facilitate, improve, support, develop, implement, and encourage; it is closely related to supply-based policy tools, suggesting the policy’s emphasis on promoting the supply of health services through various implementation and encouragement mechanisms. However, from a health equity perspective, although the policy stresses widespread service promotion, specific mechanisms for equitable distribution, particularly for addressing service gaps for different demographic groups, are lacking.
Third, the monitoring and prevention dimension includes terms such as monitoring, prevention and control, environment, region, residents, facilities, publicity, and patients. This dimension emphasizes environmental and disease monitoring and prevention, corresponding to environment-based policy tools. In terms of health equity, these policies aim to ensure public health through improvements in facilities and the environment, but they fall short of addressing the disparities between regions or resident groups, particularly those in economically disadvantaged or remote areas.
Fourth, the medical institution and management dimension consists of terms such as hospital, institution, management, department, responsible, personnel, unit, and the State Council. It reflects the policy’s focus on the construction and management of medical institutions and the enhancement of health care personnel and primary medical services. This dimension aligns with supply-based policy tools, focusing on strengthening health care infrastructure. However, from a health equity perspective, there is insufficient clarity regarding how medical resources are distributed among different socio-economic groups.
Fifth, the social participation and organization dimension includes terms such as society, organization, community, mass, and population, highlighting the role of social participation and organization in implementing universal health services. This dimension reflects efforts to achieve health equity by mobilizing broad societal engagement. However, the policy does not sufficiently elaborate on how different groups are involved in these initiatives, particularly the underrepresentation of the youth group in social participation efforts.
Sixth, the policy and system dimension involves terms such as policy, mechanism, system, planning, government, assessment, and the State Council. This dimension emphasizes the need to formulate and improve relevant policies and strengthen oversight and assessment mechanisms; it reflects both demand-based and supply-based policy tools. From a health equity perspective, while the policy framework stresses the importance of policy mechanisms, concrete strategies for ensuring equitable access to health services across diverse population groups are lacking.
Seventh, the data and information dimension includes terms such as information, data, knowledge, and technology, emphasizing the importance of data management and information sharing in enhancing health care technology applications. This dimension aligns with supply-based policy tools, highlighting the role of technology in promoting health services. However, in terms of health equity, the potential gaps in data access and application for marginalized groups are not adequately addressed in the policy.
Finally, the infrastructure and standard dimension includes terms such as foundation, grassroots, quality, industry, combination, and sports, reflecting the policy’s focus on developing infrastructure and establishing standards to promote sports and fitness activities. This dimension is related to supply-based policy tools. While the policy highlights infrastructure improvement, there is little discussion about how this will ensure equitable access for different socio-economic groups.
Additionally, Fig. 6 shows that high-frequency terms such as health, service, medical care, hygiene, and sports are grouped within the same dimension, with these terms occupying the largest nodes in the word frequency network; this indicates that the policy text places considerable emphasis on the provision of health, medical services, and sports activities. However, despite the focus on promoting and improving these fields, the policy lacks detailed implementation pathways, especially concerning the intersection of policy tools and health equity, with limited attention to equitable service distribution and resource allocation strategies across different population groups.

Corresponding analysis quadrant distribution results
Correspondence analysis
In the context of body-health integration policies, correspondence analysis helps us understand how different policy instruments—demand-based, supply-based, and environmental-based tools—interact to promote health equity. By plotting keywords based on their thematic relevance and contribution to policy outcomes, we can assess the emphasis placed on specific dimensions, such as public health services, medical institutions, and social participation. According to the results of the correspondence analysis (Fig. 6), the keywords are distributed across four quadrants, indicating different policy approaches and their alignment with health equity goals.
First quadrant
High Policy Emphasis – High Health Equity Impact. This quadrant represents areas where policy tools exert a strong influence in terms of both addressing public demand and promoting equitable health outcomes. Words in this quadrant include community, sports, medical integration, fitness for all, mass facilities, and sports events. These terms suggest that demand-based policies in this area focus on promoting physical activity through community-based services, with an emphasis on inclusive programmes that aim to improve health equity by engaging diverse populations in sports and fitness activities. The high correlation between these terms shows that policy tools are designed to integrate health and sports at the community level, fostering broad participation and equitable health outcomes.
Second quadrant
High Policy Emphasis – Low Health Equity Impact. Keywords such as information, medical services, institutional care, elderly, technology, geriatric, and medical elderly are positioned in this quadrant. These findings indicate that supply-based policy tools are focused on improving medical care for elderly individuals, especially those with chronic diseases. While the policy strongly emphasizes improving services for an ageing population, there is less consideration of equitable access across different demographic groups, particularly younger populations; this suggests a potential gap in addressing the health needs of other vulnerable groups through these supply-based measures.
Third quadrant
Low Policy Emphasis – Low Health Equity Impact. The third quadrant contains terms such as management, responsibility, safety, education, implementation, knowledge, detection, environment, disease prevention, health, hygiene, and action. These keywords reflect environment-based policy tools that emphasize public health measures such as disease prevention and hygiene education. However, the relatively low policy emphasis and health equity impact suggest that while these measures are essential, they may not yet be fully integrated or impactful in addressing disparities in health outcomes. The policy tools in this dimension focus on broad environmental health measures, but they lack targeted strategies to ensure equitable access and outcomes across different populations.
Fourth quadrant
Low Policy Emphasis – High Health Equity Impact. This quadrant includes keywords such as city, fitness, activity, citizen, unit, and adolescent. Here, environment-based policy tools are focused on urban health initiatives, such as promoting physical activity and fitness in city settings. Although these tools have strong potential to promote health equity, particularly for adolescents and city residents, the low emphasis on these policies suggests that there are gaps in fully realizing their potential. The clustering of these terms indicates a reliance on the urban public health system to promote fitness, but the policy framework may need to strengthen its focus on ensuring equitable access to fitness programmes across urban populations, especially for youths and marginalized groups.
By categorizing the keywords into four quadrants and aligning them with the X-axis (policy type) and Y-axis (health equity), we gain insights into the strengths and weaknesses of the current policy framework on body-health integration. The “high-high” quadrant indicates a strong alignment between policy tools and health equity goals, particularly in promoting inclusive sports programmes. However, the “high-low” quadrant suggests that certain supply-based policies, such as elderly care, lack equitable access for other demographic groups. Similarly, while some environment-based policies focus on broad health improvements (third quadrant), they may not yet be addressing disparities effectively. Finally, the “low-high” quadrant highlights opportunities for improving urban fitness policies to better support health equity for younger populations and citizens.
Discussion
Policy tools based on demand: the fulcrum of public health equity promotion is the goal orientation for All
Policy tools are mechanisms that effectively regulate government behaviour and clear approaches to solving public policy problems [30]. Research indicates that advancing health equity in policy formulation requires a multifaceted approach across multiple sectors. Strategies include employing various policy frameworks to engage diverse stakeholders, forming broad coalitions that extend beyond health, and prioritizing equity in the decision-making process [31]. In policy formulation, understanding the policy space that promotes health equity is essential for prioritizing equity in decision-making [32].
The objective of the integration of sports and medicine policy is to improve patient outcomes and reduce costs by combining behavioural health and physical health services. Health equity is an important goal, which requires that health services, medical services, sanitation services, etc., should be oriented towards all groups of people and that the quality and level of improvement should be ensured to achieve a fair distribution of health. At the same time, health equity also requires a rational distribution of health resources so that specific groups of people are not allowed to consume too many health resources and more people can share these resources. To that end, institutional organizations such as hospitals, institutions, and centres need to provide equal services and not provide different levels of quality of service to people due to differences in geography, economic conditions, and so on. In addition, health equity requires encouraging the participation of the entire population and promoting improvements in the health of society as a whole so that everyone can enjoy equal health treatment. Education and publicity campaigns are also important means of achieving health equity by increasing people’s health awareness and knowledge so that everyone can acquire basic health care knowledge.
Globally, many countries utilize policy tools to promote health equity and achieve universal health coverage. To promote physical activity levels and prevent the onset of non-communicable diseases in all populations worldwide, the World Health Organization (WHO) has developed a series of global recommendations and guidelines for action on healthy exercise, encouraging the integration of public health and wellness and national physical participation to promote active lifestyles. The groups covered range from children (including those under 5 years of age) to adolescents, healthy adults, and older people. Because of its functions of guidance, control, coordination, and symbolization, the policy provides practical means for the successful resolution of social problems [33]. Therefore, the realization of universal health through policy instruments is a common practice in countries worldwide. For example, in 2005, Sweden issued the Implementation Programme for Healthy Eating Habits and Promotion of Physical Education for the Public. In 2008, the United States issued the Guidelines for Physical Activity for Healthy Adults, Older Adults. In 2016, Canada issued the world’s first 24-hour activity guideline for children and youth, the 24-hour Exercise Guidelines for Children and Youth in Canada.
In China, research indicates that there are inequalities in the allocation of health resources and the utilization of health services [34]. The integration of sports and medicine policies aims to enhance the provision and outcomes of health care services by combining physical and behavioural health services [35]. Integration strategies include establishing demonstration projects, developing interdisciplinary training programmes, implementing population-based approaches, and testing innovative payment models [36]. The integration of health care is also a policy to promote national health, which falls under the category of public policy. Due to its public nature, the policy of integration enables the construction of a “healthy China”; this makes the public policy tool of integration an important fulcrum for the promotion of health equity. So, does the policy take into full consideration the needs and special circumstances of socially disadvantaged groups and help reduce their health inequalities?
In this regard, through text analysis, the policy tool of physical and medical integration aims to promote health equity by covering all people in the policy tool. Health for all refers to the health of all people, and all people include all ethnic groups in China and all types of people, including men and women, both old and young. The deep integration of national fitness and national health aims to actively respond to the national strategy of national fitness and promote the construction of a healthy China. Currently, medical and health resources are relatively scarce, and providing a supply that is commensurate with current health needs is difficult, which poses a major problem for China’s health work. The integration of sports and medicine utilizes sports and exercise to regulate and protect national health to a certain extent. Table 1 shows that the keywords country, China, hospital, all people, society, institution, health, people, public, children, students, disabled, women, and elderly account for 21.88% of all keywords, which indicates that the policy of the integration of sports and medicine is aimed at realizing the health of all people; this means that all populations are beneficiaries, and everyone, regardless of age, gender, occupation, etc., has the opportunity to receive support for health management and disease prevention through the services of body-health integration. In addition, in terms of special populations, the policy on the integration of sports and health care focuses on the prevention and treatment of chronic diseases, and people suffering from such diseases can receive better treatment and rehabilitation support through exercise prescriptions and personalized health management services. Moreover, in terms of health practitioners, the policy on the integration of sports and medicine provides health practitioners such as clinicians, health managers, and rehabilitation physicians with opportunities for development and cooperation, enabling them to provide scientifically accurate exercise prescriptions and comprehensive health management services. In other words, the ultimate goal of the policy on the integration of physical medicine is universal coverage of health, meaning that all people can enjoy health and wellness services that are equitably accessible, of high quality, and efficient.
Supply-based policy tools: the integration of physical medicine is an important pathway for promoting health equity
China is actively addressing the challenges of its rapidly ageing population through integrated health and care policies. The government has implemented a top-down approach, focusing on integrating health and care services at the institutional and community levels, piloting long-term care insurance, and reforming administrative structures [37]. The sports-health integration policy aims to promote collaboration between the sports and medical sectors to improve public health and prevent diseases, particularly among elderly individuals [38].
The term “sports-medicine integration” refers to a model that utilizes sport and physical education in conjunction with medical treatment to promote health. This means that under the guidance of policies, government departments effectively integrate the tangible and intangible resources of the sports system and the medical and health care system to achieve the service mode and process of enhancing people’s physical fitness and improving their health through the extensive participation of the general public [39]. Thus, the policy of the integration of sports and medical care, which involves the comprehensive use of multiple elements of sports and medical care, not only has but also can play a positive role in the prevention and rehabilitation of chronic diseases, such as health promotion.
By using the high-frequency word statistics function of KH Coder, this study finds that the words in the category of health and hygiene are related to the content of health and hygiene fields, whereas the words in the category of society and the state reflect the relationship between policies and the overall development of society. The policy implementation method ultimately shows that service, medical care, management, technology, related, standard, system, promotion, nutrition, fitness, action is the first most common, accounting for 13.84% of all high-frequency words (Table 3). According to Fig. 5, the related vocabulary of these high-frequency words can be summarized in terms of policy in combination with the content. The words in the category of development and promotion indicate that the main goal of the policy is to promote the development of health and hygiene, whereas the words in the category of service and provision emphasize that the policy should provide services and implement measures to improve health and hygiene. The words in the category of technology and resources highlight the attention and use of technology and resources in policy, whereas the words in the category of management and mechanisms relate to the management and institutional aspects of policy. Finally, the words in the category of construction and improvement emphasize the need for policies to establish a sound and relevant system to promote the development of health. The analysis of high-frequency words shows that health, services, medical care, health, sports, and institutions are the most important keywords in the related vocabulary, reflecting the fact that the policy pays more attention to the public and fairness of the supply and distribution of health-centred services. Equitable resource allocation and service realization are guaranteed.
Public sports products and medical services are supplied mainly by government-led organizations; thus, policy implementation and the integration of regulations are key. The integration of sports and medical care requires sectoral integration, policy and regulation integration, resource supply and demand integration, and professional talent integration. Sports medical and health resources are an important part of public service resources, and their attribute of being quasi-public goods determines the balanced allocation of sports medical and health resources. However, in practice, the differences in the allocation of physical and medical resources between regions, urban areas and rural areas, and populations have led to an imbalance in the supply structure of physical and medical health services. Thus, policy tools are needed to ensure equitable resource allocation and services. Sports and medical and health resources should be promoted for rural, remote, and disadvantaged groups, and balanced development should be promoted. Thus, the core content and goal of China’s sports and medical integration policy are to provide comprehensive health services by promoting the development of health and hygiene, utilizing technology and resources, establishing a perfect management mechanism, and promoting improvements in the health level of the whole population to achieve the goal of health equity. Moreover, the relevant policy defines guidelines for physical fitness activities; establishes a comprehensive library of exercise prescriptions for different populations, environments, and physical conditions; and is thus an important pathway for promoting health equity.
Environment-based policy instruments: collaborative governance as a pathway for health equity promotion
The government has adopted a top-down approach, employing pilots and demonstrations to establish aftercare facilities, integrate service delivery, and introduce long-term care insurance [37]. The integration of sports and medicine (ISM) programme has been implemented in cities such as Suzhou and Shanghai, aiming to alleviate the contradiction between health needs and medical supply [40]. Policy analysis reveals a transition from mandatory to voluntary or hybrid policy tools, with a need for more attention to specific service groups and sports risk assessment [41]. The Luohu model, which is an integrated urban health care system, has improved care integration and patient satisfaction but faces challenges in aligning with payment reforms [42]. These initiatives demonstrate China’s efforts to create a more comprehensive and integrated health care system.
Sports integration involves many sectors and stakeholders and requires the coordination and cooperation of government departments, sports management organizations, the education sector, health care institutions, and other parties. However, there may be difficulties in communication and coordination between different departments, which may affect the effectiveness of policy implementation due to issues such as the distribution of interests and unclear powers and responsibilities. Governmental departments need to change their concepts, re-conceptualize the value and function of the integration of sports and medical care for health promotion, integrate the relevant resources of various departments, and leverage the synergistic effects of publicity, sports, medical care and health care, education, and other relevant departments. The combination and mutual supplementation of the sports sector and the medical and health sector are an important foundation for enhancing health equity, especially the health strategy that emphasizes early health and zero-level prevention, and a consensus has been reached regarding the promotion of the community’s body-medicine integration to cover the front and back end of the health of the mixed health model [39]. The purpose of body-medicine integration is to build a management mechanism that links the sports sector with the medical and health sectors. The synergistic governance of body-medicine integration involves the deep integration of sports, medical care, health, education, and other fields through the full cooperation of multiple subjects to promote health. In addition, some scholars have proposed that through resource integration and mutual synergy, health resource allocation can be optimized, health service efficiency can be improved, and ultimately, the health level of the whole population can be promoted; as a result, the level of equalization of public sports and health services can be improved [43].
At the governmental level, the highest government and local governments assume different but interrelated roles in the development of body-medicine integration policies to jointly promote the development of China’s body-medicine integration and to provide people with better quality health services and medical resources. The top governments, such as the State Council and the central government, play strategic decision-making and overall planning roles in the development of policies for the integration of sports and medicine. This is reflected mainly in strategic planning, formulating policy guidance, and coordinating and improving laws and regulations. Local governments play a territorial and executive role in the development and implementation of body-medicine integration policies. They need to formulate body-medicine integration policies that are appropriate for their region based on the strategic planning and policy guidance of the supreme government and considering local realities.
At this level, the high-frequency words (Table 3) mode, sport, promote, safety, activity, level, policy, resources, sector, and project can be categorized as associated words from the policy objective dimension of the policy objective latitude policy objective dimension, accounting for 42.37% of the frequency of all words. The high-frequency words appearing in Figs. 5 and 6, namely, establish, develop, implement, promote, improve, encourage, provide, strengthen, and carry out, reflect the determination of the state to formulate local policies, integrate resources, and promote the implementation of the specific goals to be achieved in the formulation of the policy on the integration of physical and medical care. The policy objectives include improving the health of the entire population, reducing the incidence of chronic diseases, and optimizing the allocation of medical resources. By analysing the policy objectives, the relevance and feasibility of the policy can be assessed.
This collaborative governance system emphasizes physical activity as an important means of health promotion, and it deeply integrates health care and non-medical means of sports, especially to address health problems caused by insufficient physical activity and social problems such as the excessive financial burden of health care caused by health. This comprehensive cooperative order not only builds an overall balanced governance environment and clarifies the rights and responsibilities of different stakeholders but also creates an important foundation for health equity.
Policy recommendations
Through a health equity lens, rural areas and synergies between rural areas, sports, health, and other functional systems are a concern for future policy development. Based on the results of these analyses, future policy recommendations for the integration of sports and health are proposed to facilitate the development and implementation of better policies for the integration of sports and health. First, resources for health and sports in rural areas should be provided. Policy tools could focus on how to improve medical facilities and sports facilities in rural areas to ensure that rural residents have access to basic medical services and opportunities for physical activity. The establishment of multi-functional community health centres that provide not only basic medical services but also sports and health education to increase health awareness and opportunities for rural residents should be supported. Second, cross-sectoral synergy should be promoted. Policies to promote synergies between the health and sport sectors should be developed; this can include resource sharing, collaborative programmes, and cross-training to improve the integration of services. Policy tools to encourage cross-sector collaboration could set incentives or provide funding to support cross-cutting programmes. Third, health education and preventive measures should be supported. Policy tools for health integration can focus on providing health education and preventive measures to reduce the incidence of chronic diseases, especially in rural areas. Emphasis on health awareness and lifestyles in physical activities should be encouraged to reduce health inequalities. Fourth, data collection and monitoring should be carried out. Health and sport data systems should be established to better monitor health inequalities and the impact of policies. Data sharing and collaboration should be promoted to ensure that information on health and sports provides useful insights for policy-makers, researchers, and communities. Fifth, community engagement and feedback mechanisms should be constructed. Policies should be developed to encourage community participation and feedback to ensure that policy tools are developed and implemented while considering the needs and opinions of residents. Health and physical education advisory committees, including rural residents and experts in related fields, should be established so that they participate in the policy decision-making process. Sixth, fund allocation and support should be considered. Sufficient funds should be allocated for health and sports programmes in rural areas to reduce health inequalities. Funding and support should be provided to train health and sports practitioners, especially in rural areas, to enhance their professional competence. In summary, through these policy tools, it is possible to promote the effective implementation of the policy of the integration of sport and physical education in rural areas while focusing on health equity to ensure that more people can benefit from and enjoy equal access to health and physical education opportunities; this will help reduce health disparities between urban and rural areas and between different social groups.
Conclusion
The integration of sports and medicine policy is a critical response to the increasing prevalence of chronic diseases in China, which can be attributed to lifestyle changes stemming from rapid socio-economic development. While the policy does not explicitly address health equity, its objectives align closely with the principles of equitable health access for all individuals. The emphasis on equitable resource allocation highlights the potential of this policy to promote health equity.
However, to fully achieve the policy’s aims, continuous improvements in implementation and monitoring are essential. Future research and policy initiatives must prioritize health equity and enhance integration strategies to more effectively cater to the diverse needs of various population groups, including policy beneficiaries, implementers, and affected communities.
Moreover, non-medical health intervention policies—such as health education and dietary guidance—can complement this health-focused approach by reducing the overuse of medical resources and ensuring equitable access to health services. The commitment of the Chinese government to support vulnerable groups, particularly in rural and impoverished areas, reflects a comprehensive strategy to address health disparities. By strengthening grassroots health care infrastructure and providing free medical services, the government aims to ensure health equity for all citizens, thereby fostering a healthier and more equitable society.
Limitations of the study
This study has certain limitations. Although it uses topic modelling to extract and summarize policy actions, resulting in some quantitative metrics (such as the number of short phrases), it remains largely a descriptive presentation and does not analyse or test the relationship between policies and health equity outcomes. Future research should further explore the potential of text analysis techniques, approaching the issue from a perspective that facilitates effectiveness evaluation, thereby deepening the analysis.
Data availability
The text data supporting this article comes from the official government website and belongs to the category of public affairs disclosure.
References
Denier Y. On personal responsibility and the human right to healthcare. Camb Q Healthc Ethics. 2005;14:224–34.
Dhaliwal LK. Health equity and sustainable development goals: role and the complexity. In: Filho WL, Wall T, Azul AM, Brandli L, Özuyar PG, editors. Good health and well-being. Cham: Springer; 2020. pp. 316–24.
Bradley BD, Jung T, Tandon-Verma A, Khoury B, Chan TCY, Cheng YL. Operations research in global health: a scoping review with a focus on the themes of health equity and impact. Health Res Policy Syst. 2017;15:32.
Walker SC, White J, Rodriguez V, Turk E, Gubner N, Ngo S, et al. Cocreating evidence-informed health equity policy with community. Health Serv Res. 2022;57(Suppl 1):137–48.
World Health Organization. World health statistics 2020: monitoring health for the SDGs, sustainable development goals. Geneva: World Health Organization; 2020.
Li XM, Kou J, Yu Z, Xiao YY, Meng Q, He LP. Health equity of rural residents in southwest China. Front Public Health. 2021;9:611583.
Fang EF, Xie C, Schenkel JA, Wu C, Long Q, Cui H, et al. A research agenda for ageing in China in the 21st century (2nd edition): focusing on basic and translational research, long-term care, policy and social networks. Ageing Res Rev. 2020;64:101174.
Wang L, Wang Z, Ma Q, Fang G, Yang J. The development and reform of public health in China from 1949 to 2019. Global Health. 2019;15:45.
Hu L, Glavin YW, Yan R, Pei C, Yan M, Zhang Y, et al. Integrating health and care in China: lessons learned and future outlook. Int J Integr Care. 2021;21:18.
Li L, Fu H. China’s health care system reform: progress and prospects. Int J Health Plann Manage. 2017;32:240–53.
Li X, Krumholz HM, Yip W, Cheng KK, De Maeseneer J, Meng Q, et al. Quality of primary health care in China: challenges and recommendations. Lancet. 2020;395:1802–12.
Fichtenberg C, Delva J, Minyard K, Gottlieb LM. Health and human services integration: generating sustained health and equity improvements: an overview of collaborations, partnerships, and other integration efforts between health care and social services organizations. Health Aff. 2020;39:567–73.
Glandon D, Mondal S, Okeyo I, Zaidi S, Khan MS, Dar O, et al. Methodological gaps and opportunities for studying multisectoral collaboration for health in low- and middle-income countries. Health Policy Plan. 2019;34:ii7–17.
Koyama M. Nurse advocacy: adopting a health in all policies approach. Online J Issues Nurs. 2018;23:1–12.
Cole M, Holland CJ, Cassius T. Inequalities across the physical activity landscape: the need for ‘structural humility’ to optimise sports and exercise medicine. Br J Sports Med. 2023;57:834–5.
Purnell TS, Calhoun EA, Golden SH, Halladay JR, Krok-Schoen JL, Appelhans BM, et al. Achieving health equity: closing the gaps in health care disparities, interventions, and research. Health Aff. 2016;35:1410–5.
Warburton DE, Nicol CW, Bredin SS. Health benefits of physical activity: the evidence. CMAJ. 2006;174:801–9.
Bali AS, Ramesh M. Designing effective healthcare: matching policy tools to problems in China. Public Adm Dev. 2017;37:40–50.
Bali AS, Howlett M, Lewis JM, Ramesh M. Procedural policy tools in theory and practice. Policy Soc. 2021;40:295–311.
Hasson RE, Brown DR, Dorn J, Barkley L, Torgan C, Whitt-Glover M, et al. Achieving equity in physical activity participation: ACSM experience and next steps. Med Sci Sports Exerc. 2017;49:848–58.
Nunes R. Fair equality of opportunity in healthcare. Conatus J Philos. 2018;3:83–97.
Chauhan UPS. History matters: role of time in policy making and analysis. Int J Hist Insight Res. 2022;8:1–7.
Berman A. Between participation and capture in international rule-making: the WHO framework of engagement with non-state actors. Eur J Int Law. 2021;32:227–54.
Batterbury SCE. Principles and purposes of European Union Cohesion policy evaluation. Reg Stud. 2006;40:179–88.
Ise OA. Integration and analysis of unstructured data for decision making: text analytics approach. Int J Open Inf Technol. 2016;4:82–8.
Maslennikova YS, Bochkarev VV, Belashova IA. Cluster analysis of word frequency dynamics. J Phys Conf Ser. 2015;574:012120.
Murtagh F. The correspondence analysis platform for uncovering deep structure in data and information. Comput J. 2010;53:304–15.
Žlahtič B, Kokol P, Vošner HB, Završnik J. The role of correspondence analysis in medical research. Front Public Health. 2024;12:1362699.
Rothwell R. Reindustrialization and technology: towards a national policy framework. Sci Public Policy. 1985;12:113–30.
Lascoumes P, Le Galès P. Introduction: understanding public policy through its instruments—from the nature of instruments to the sociology of public policy instrumentation. Governance. 2007;20(1):1–21.
Townsend B, Friel S, Freeman T, Schram A, Strazdins L, Labonte R, et al. Advancing a health equity agenda across multiple policy domains: a qualitative policy analysis of social, trade and welfare policy. BMJ Open. 2020;10:e040180.
Campbell F, Sein TT, Htoo TS, Khine WYK, Howard N, Balabanova D. Policy space and pro-health equity national policymaking: a case study of Myanmar during political transition (2006-16). Health Policy Plan. 2023;38:170–80.
Christensen T, Ma L. Coordination structures and mechanisms for crisis management in China: challenges of complexity. Public Organ Rev. 2020;20:19–36.
Zhang X, Zhao L, Cui Z, Wang Y. Study on equity and efficiency of health resources and services based on key indicators in China. PLoS ONE. 2015;10:e0144809.
Wang B, Lin Q, Wang Y, Tang S. Policy analysis of the integration of sports and medicine against the backdrop of “healthy China”: a qualitative study using NVivo. Int J Environ Res Public Health. 2023;20:2079.
Ader J, Stille CJ, Keller D, Miller BF, Barr MS, Perrin JM. The medical home and integrated behavioral health: advancing the policy agenda. Pediatrics. 2015;135:909–17.
Hu B, Guo H, Zhou P, Shi ZL. Characteristics of SARS-CoV-2 and COVID-19. Nat Rev Microbiol. 2021;19:141–54.
Xu M, Ng WC, Lim WYB, Kang J, Xiong Z, Niyato D, et al. A full dive into realizing the edge-enabled metaverse: visions, enabling technologies, and challenges. IEEE Commun Surv Tutor. 2022;25:656–700.
Dover DC, Belon AP. The health equity measurement framework: a comprehensive model to measure social inequities in health. Int J Equity Health. 2019;18:36.
Zhang H, Wu C, Zhang Z, Zhu Y, Lin H, Zhang Z et al. ResNeSt: split-attention networks. In: Proceedings of the IEEE/CVF conference on computer vision and pattern recognition. New Orleans: IEEE; 2022. pp. 2736-46.
Tsao CW, Aday AW, Almarzooq ZI, Anderson CAM, Arora P, Avery CL, et al. Heart disease and stroke statistics-2023 update: a report from the American Heart Association. Circulation. 2023;147:e93–621.
Chou CH, Shrestha S, Yang CD, Chang NW, Lin YL, Liao KW, et al. miRTarBase update 2018: a resource for experimentally validated microRNA-target interactions. Nucleic Acids Res. 2018;46:D296–302.
Liu Z, Zhang S, Li L, Hu B, Liu R, Zhao Z, et al. Research on the construction and prediction of China’s national fitness development index system under social reform. Front Public Health. 2022;10:878515.
Acknowledgements
We wish to thank all organizations and individuals involved in the funding, planning, design, and conducting of this research.
Funding
This work was financially supported by the Higher Education Research Project of Heilongjiang Higher Education Association (23GJYBJ058), the Harbin Institute of Physical Education Introduction of Talent Research Start-up Project (RC21-20224), and the 2024 Zhaoqing Philosophy and Social Sciences Planning Project (Co-construction of Disciplines) (24GJ-71).
The research was funded by the Macao Science and Technology Development Fund (FDCT) under Grant(No. 0071/2023/RIB3 & No.0003-2024-AGJ)
Author information
Authors and Affiliations
Contributions
M. Z. and L. Y. contributed equally to the study. M. Z. and L. Y. wrote the main manuscript. B. Q. performed the data analysis. Y. Y. and G. W. revised the manuscript. C. L. prepared an outline, supervised, and performed the final revision of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Zhao, M., Yang, L., Qian, B. et al. Physical-medical integration policies and health equity promotion in China: a text analysis based on policy instruments. Int J Equity Health 23, 266 (2024). https://doiorg.publicaciones.saludcastillayleon.es/10.1186/s12939-024-02327-9
Received:
Accepted:
Published:
DOI: https://doiorg.publicaciones.saludcastillayleon.es/10.1186/s12939-024-02327-9